RYBREVANT FASPRO™ vs RYBREVANT® (amivantamab-vmjw)RYBREVANT FASPRO™ vs RYBREVANT® (PALOMA-3)

Study Design
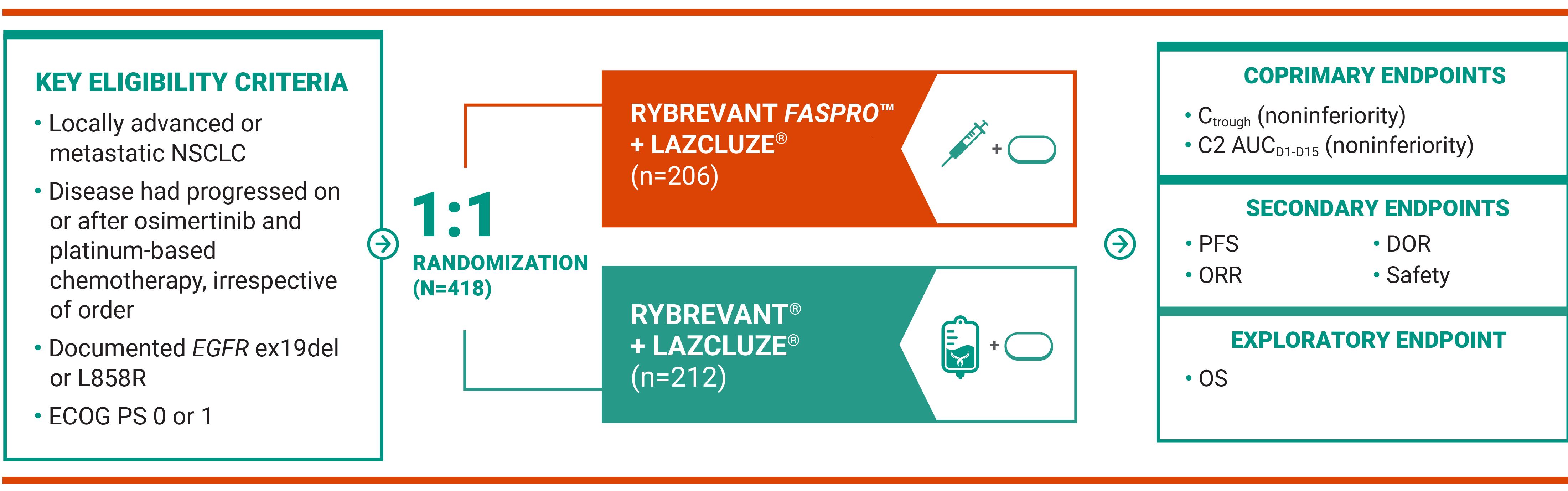
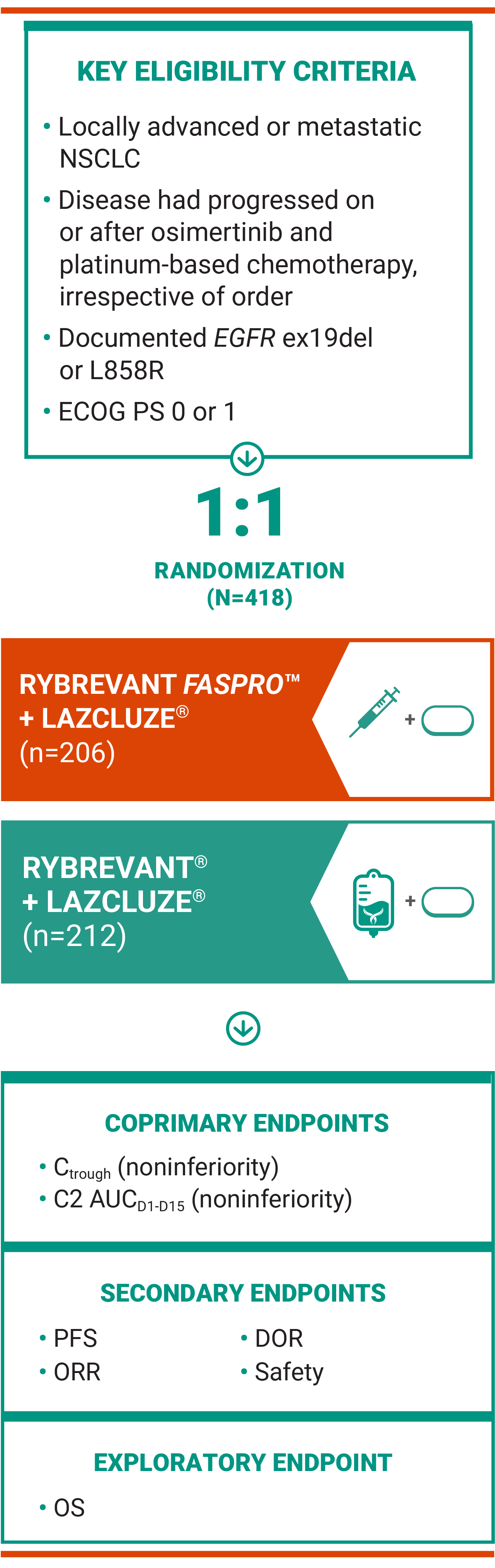
RYBREVANT FASPRO™ is approved across all RYBREVANT® indications as a rapid, ~5-minute subcutaneous injection1*
PALOMA-3: A phase 3, randomized, open-label trial evaluated pharmacokinetics (PK) of RYBREVANT FASPRO™ vs RYBREVANT®, both in combination with LAZCLUZE® (lazertinib)1,2
*Administration time only; actual clinic time may vary.
RYBREVANT FASPRO™ effectiveness has been established based on studies of RYBREVANT®1
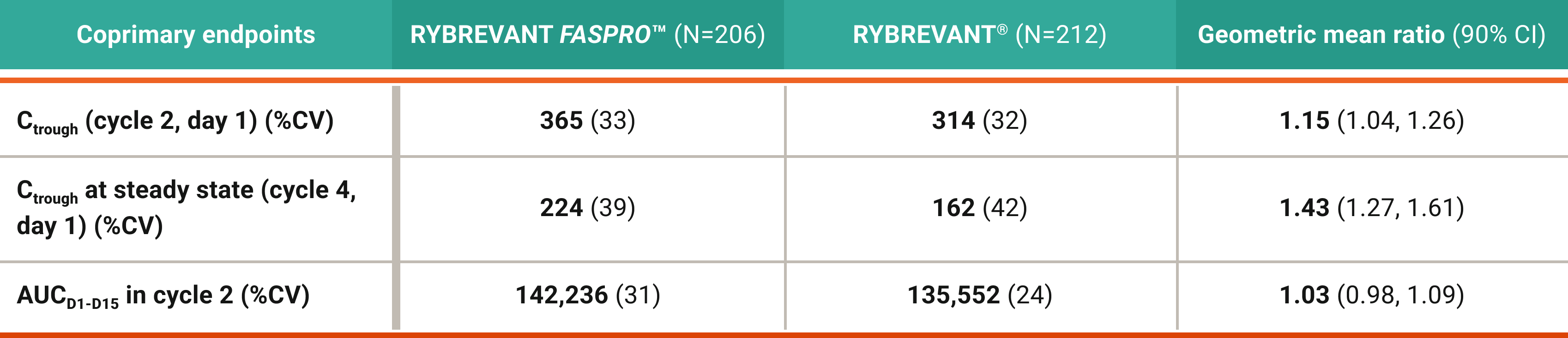
RYBREVANT FASPRO™ demonstrated a comparable PK profile to RYBREVANT®2

AUC, area under the curve; C, cycle; Ctrough, trough concentration; CI, confidence interval; CV, coefficient of variation; D, day; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; ex19del, exon 19 deletion; NSCLC, non–small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival.
Safety
Safety profile of RYBREVANT FASPRO™ vs RYBREVANT® arm in the PALOMA-3 trial
Lower rates of administration-related reactions (ARRs) observed with RYBREVANT FASPRO™1*
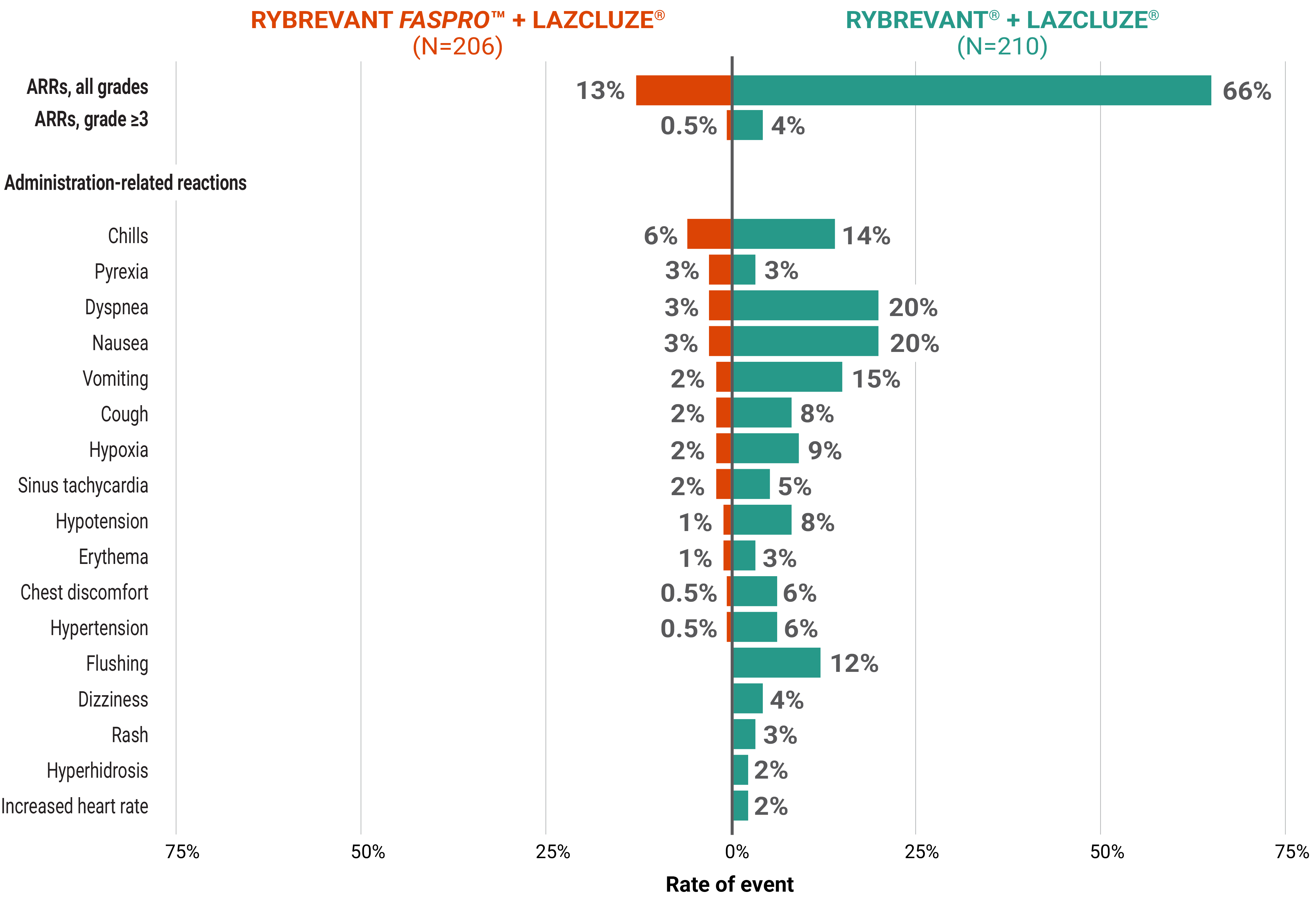
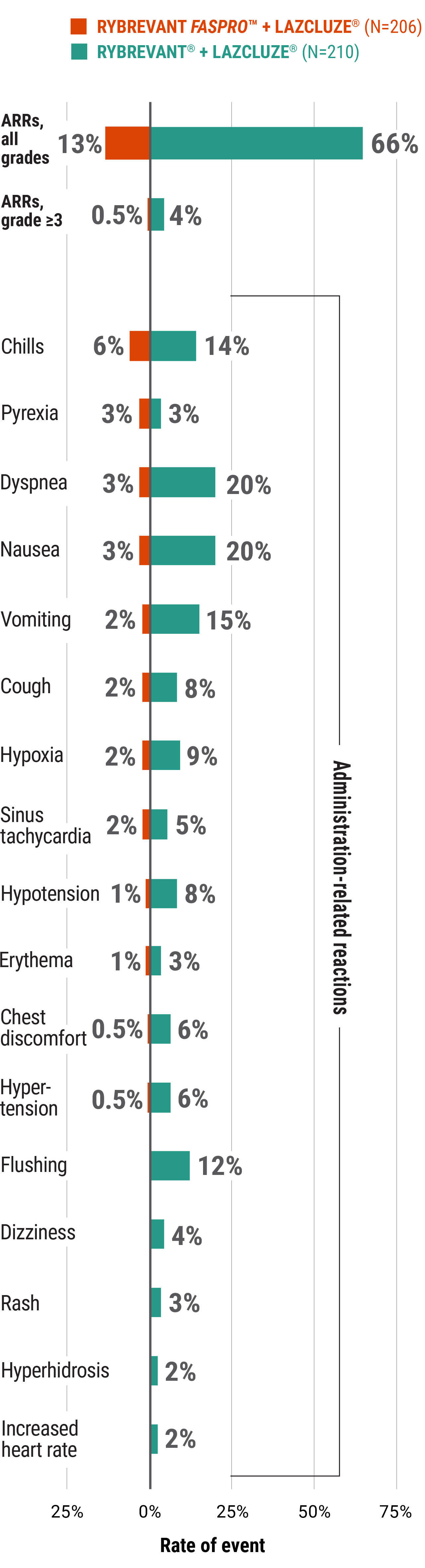
89% of ARRs in PALOMA-3 occurred on week 1, day 1, and median onset time of ARRs is ~2 hours. Monitor patients for any signs and symptoms of ARRs during injection in a setting where cardiopulmonary resuscitation medication and equipment are available. Patient monitoring time is up to healthcare provider discretion.1
*In clinical trials of RYBREVANT® and the Prescribing Information for RYBREVANT®, the term “infusion-related reactions” was used instead of “administration-related reactions.”
Low rates of VTE observed with RYBREVANT FASPRO™ and prophylactic anticoagulant use2
80% (n=164) of patients in the RYBREVANT FASPRO™ + LAZCLUZE® arm of PALOMA-3 received prophylactic anticoagulation for the first 4 months of treatment. Among all patients receiving RYBREVANT FASPRO™ + LAZCLUZE® (N=206), VTE rate was 11%.1,2
Majority of ARs were grades 1 and 21
ARs (≥10%) in PALOMA-31
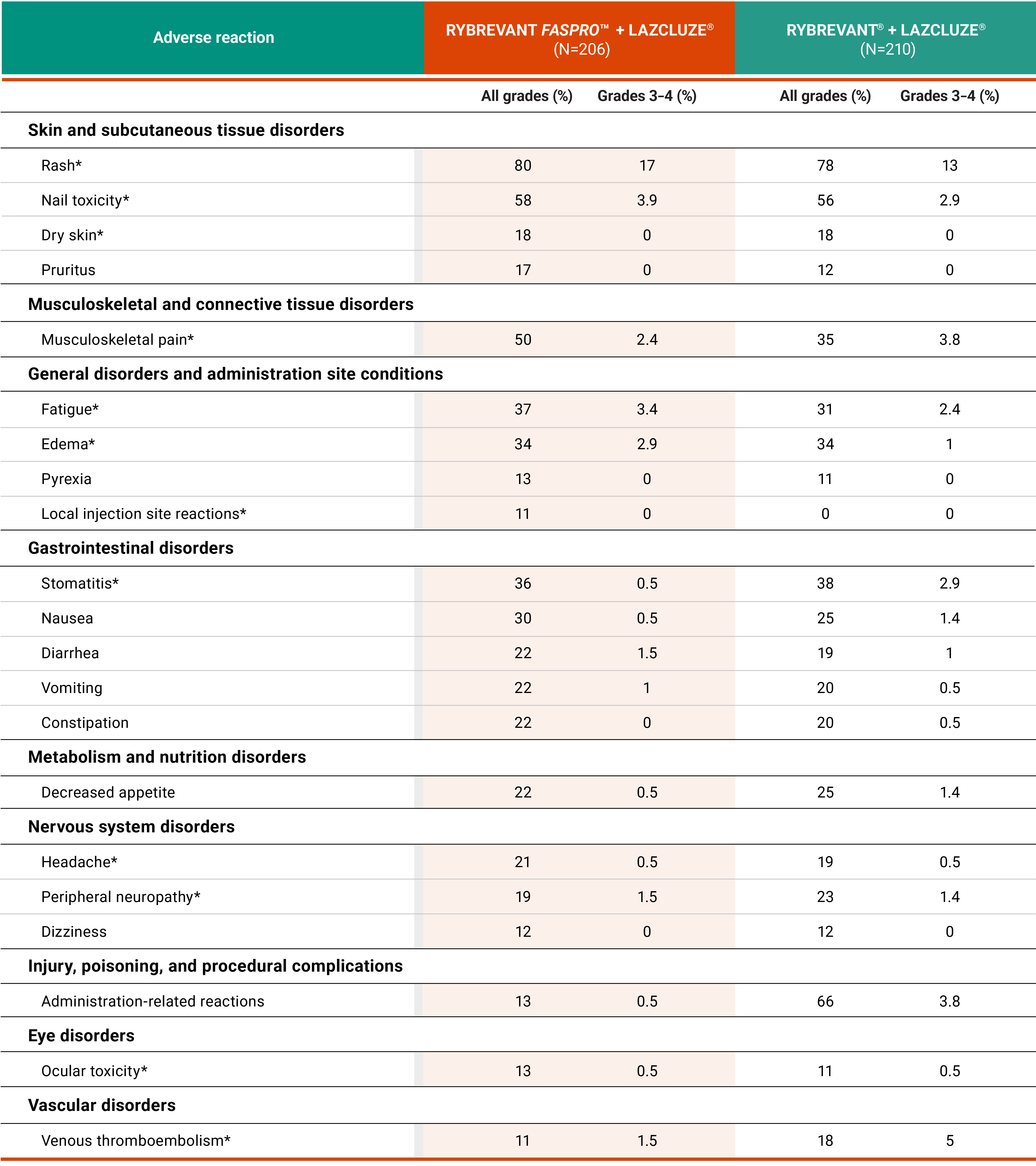
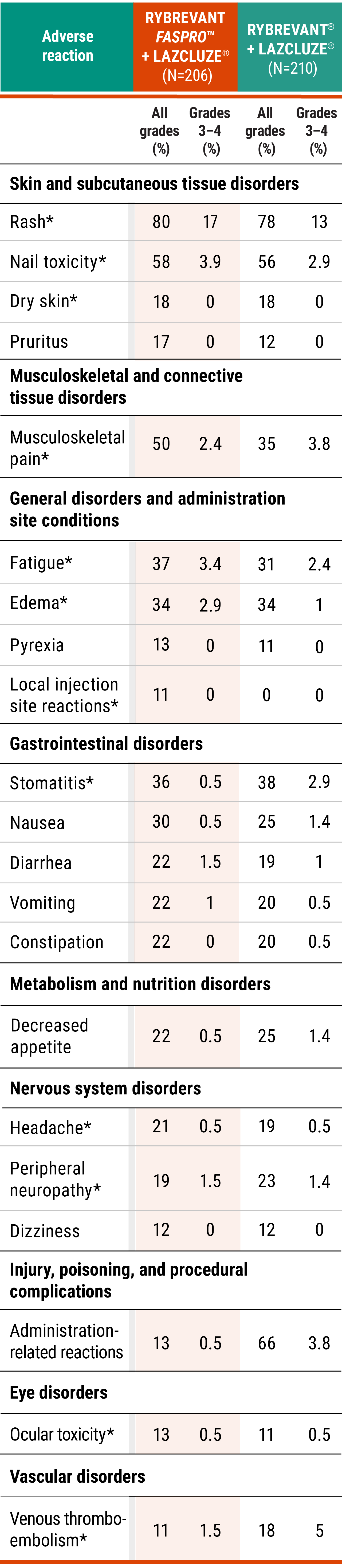
*Grouped terms.
- Serious ARs occurred in 33% of patients who received RYBREVANT FASPRO™ + LAZCLUZE®1
- Serious ARs in ≥2% of patients who received RYBREVANT FASPRO™ + LAZCLUZE® included ILD/pneumonitis (6%), pneumonia (2.4%), VTE (2.4%), and fatigue (2.4%)1
- Death due to ARs occurred in 5% of patients treated with RYBREVANT FASPRO™, including ILD/pneumonitis (1.9%), pneumonia (1.5%), respiratory failure (1%), and sudden death (1%)1
- The most common ARs (≥20%) were rash, nail toxicity, musculoskeletal pain, fatigue, stomatitis, edema, nausea, diarrhea, vomiting, constipation, decreased appetite, and headache1
- Clinically relevant ARs in <10% of patients who received RYBREVANT FASPRO™ + LAZCLUZE® were abdominal pain, hemorrhoids, ILD/pneumonitis, and skin ulcer1
Select laboratory abnormalities (≥20%) that worsened from baseline in PALOMA-31*
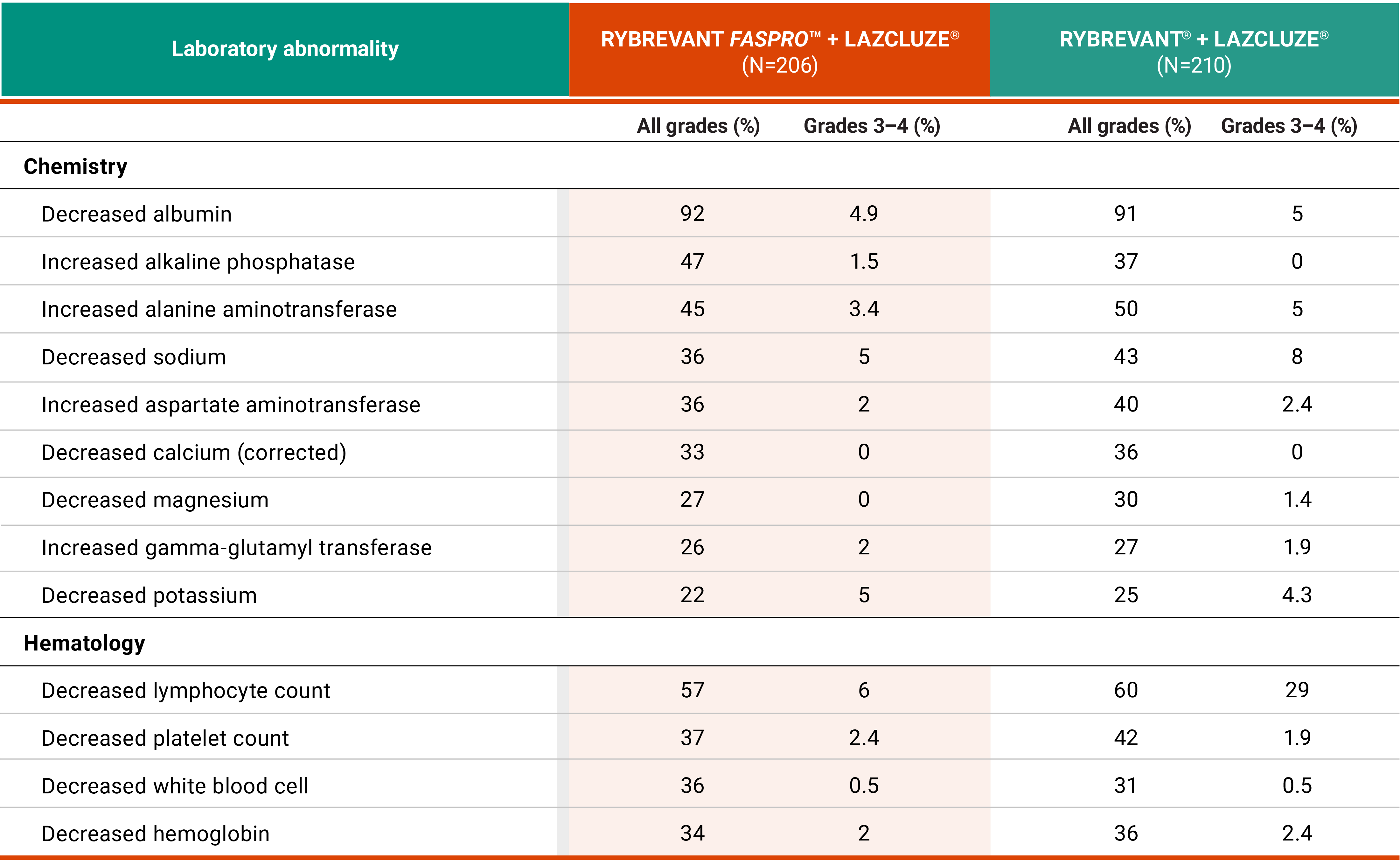
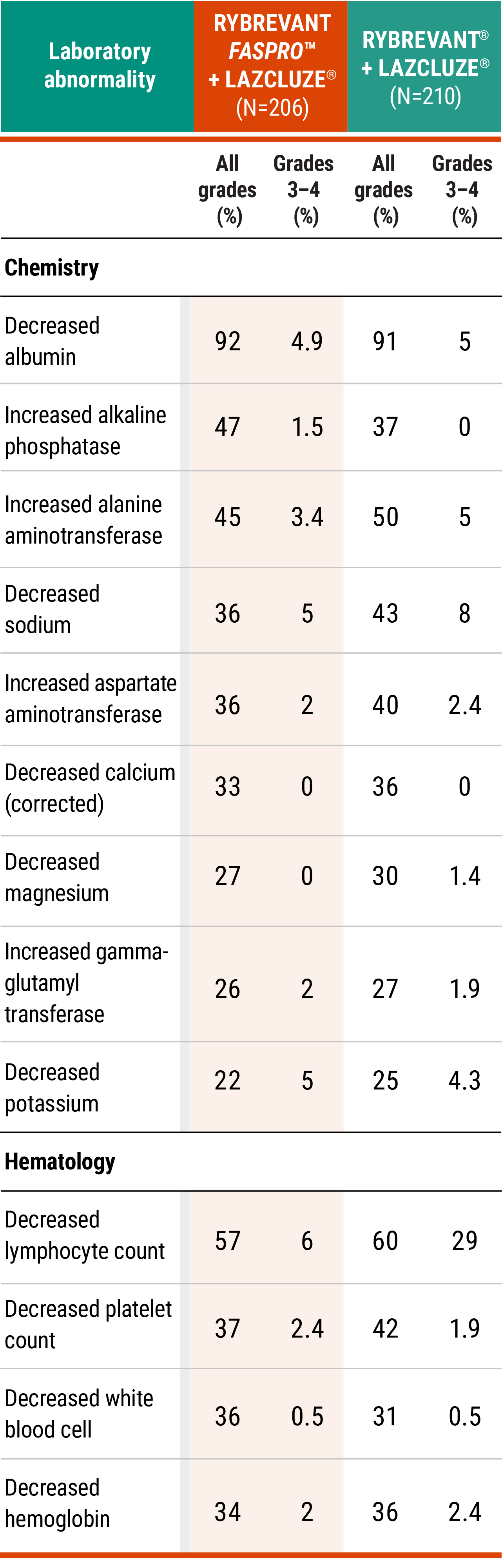
*The denominator used to calculate the rate is the number of patients with a baseline value and at least one post-treatment value for the specific lab test.
Prophylaxis may help reduce the risk of key ARs
Learn moreDiscontinuation rates and dose modifications
- Permanent discontinuation of RYBREVANT FASPRO™ due to an AR occurred in 13% of patients1
- Dosage interruptions of RYBREVANT FASPRO™ due to an AR occurred in 54% of patients1
- Dose reductions of RYBREVANT FASPRO™ due to an AR occurred in 20% of patients1
Adaptable dosing is available to help your patients manage ARs and stay on treatment4*
Learn more*Certain types and severity of ARs require discontinuation after first occurrence.1
AR, adverse reaction; ILD, interstitial lung disease; VTE, venous thromboembolism.
References:
- RYBREVANT FASPRO™ [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Leighl NB, Akamatsu H, Lim SM, et al. Subcutaneous versus intravenous amivantamab, both in combination with lazertinib, in refractory epidermal growth factor receptor–mutated non–small cell lung cancer: primary results from the phase III PALOMA-3 study. J Clin Oncol. 2024;42(30):3593-3605. doi:10.1200/JCO.24.01001
- Yang R, Wang H, Liu D, Li W. Incidence and risk factors of VTE in lung cancer: a meta-analysis. Ann Med. 2024;56(1):1-14. doi:10.1080/07853890.2024.2390200
- Data on file. Janssen Biotech, Inc.