RYBREVANT® (amivantamab-vmjw)PROACTIVE THERAPY MANAGEMENT

Overview
Use proactive therapy management to help optimize outcomes1
Studies incorporating proactive therapy management demonstrated significantly reduced rates of key ARs2,3
Initiate prophylactic glucocorticoids
prior to first infusion
design
22.5%
rate of IRRs1,3
Rate of IRRs (%)
week 1, day 1
Initiate prophylactic antibiotics
with skincare management
design
44%
reduction in grade ≥2 key dermatologic ARs
with antibiotics and skincare management2
Rate of grade ≥2 key
dermatologic ARs (%)
details
Initiate anticoagulants
when combined with LAZCLUZE® (lazertinib)
design
5%
rate of VTE when using anticoagulants
for the first 4 months of treatment with RYBREVANT® + LAZCLUZE®2,4*
Rate of VTE (%)
†~97% of patients in the RYBREVANT® + LAZCLUZE® arm of MARIPOSA did not receive prophylactic anticoagulation for the first 4 months.1
*Among all COCOON study participants, the VTE incidence was 11% (n=18/170) from 5 to 8 months.2
AR, adverse reaction; IRR, infusion-related reaction; VTE, venous thromboembolism.
Protocol
Proactive strategies that may help patients start and stay on RYBREVANT® + LAZCLUZE®
IRR premedications5
Glucocorticoid
(week 1, days -2
and -1, and day 1
an hour before
first infusion*)
Antihistamine and antipyretic prior to each infusion
Month
1
2
3
4
5
6
7
At-home treatment protocol
VTE prophylaxis2,5,6
Months 1–4: Anticoagulation
(eg, DOACs or LMWHs)†
COCOON dermatologic prophylaxis2,5
Months 1–3: Doxycycline or minocycline 100 mg twice daily
Months 4–12: Topical clindamycin 1% lotion
on the scalp before bedtime
Daily: Ceramide-based moisturizer
on the body and face at least once daily
Daily: Wear protective clothing and broad-spectrum sunscreen
(SPF ≥30)
Daily: Chlorhexidine 4% wash
on fingernails and toenails for paronychia
Month = month of treatment with RYBREVANT® and LAZCLUZE®.
*Optional for subsequent doses.5
†NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommendations for cancer-associated VTE disease: anticoagulant options for VTE prophylaxis for ambulatory patients with cancer include DOACs and LMWHs.6‡
‡Recommendations derived from clinical trials of ambulatory patients with cancer with high thrombosis risk (>18 years, Khorana VTE Risk Score of ≥2, initiating new course of chemotherapy) and are not included in product labeling. Prophylaxis duration should be 6 months or longer if risk persists.6
DOAC, direct oral anticoagulant; IV, intravenous; LMWH, low molecular weight heparin; NCCN, National Comprehensive Cancer Network; SPF, sun protection factor.
Expand to learn more about the impact of prophylaxis and recommended protocols
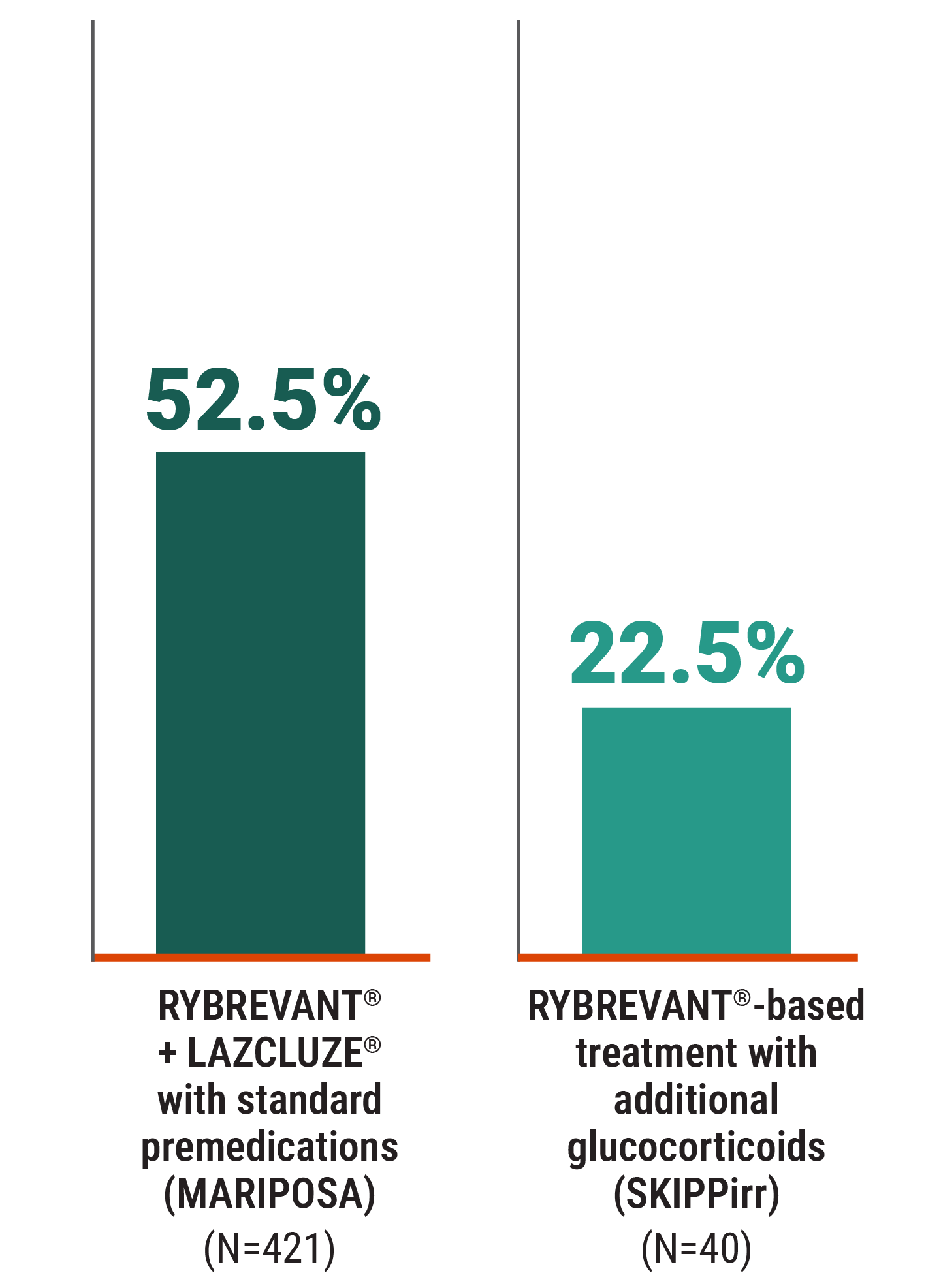
Premedicate with glucocorticoids prior to first infusion to reduce IRRs
Please refer to the full Prescribing Information for RYBREVANT® for recommended IRR premedications throughout treatment.
SKIPPirr is a phase 2 prospective study assessing prophylactic strategies to reduce incidence and/or severity of first-dose IRRs with RYBREVANT®, with the dexamethasone 8 mg cohort reaching the expansion stage.* The primary endpoint is the incidence of IRR events on week 1, day 1. Limitations of the study include that SKIPPirr is not a comparative study and dexamethasone 8 mg oral cohort sample size is n=40.3
SKIPPirr protocol:
On week 1, day -2 and day -1, patients received dexamethasone 8 mg oral twice daily (16 mg daily dose).† On week 1, day 1, patients received dexamethasone 8 mg oral and 10 mg IV 1 hour prior to infusion, in addition to an antihistamine and antipyretic.3
*This was a Simon 2-stage design. Stage 1 n=6. Stage 2 n=16. Expansion stage n=40. See full presentation for more details.3
†In the Prescribing Information for RYBREVANT®, the week 1, day 1 dexamethasone dose is 20 mg IV.5
All-grade IRRs on week 1, day 1 infusion (%)1,3,7




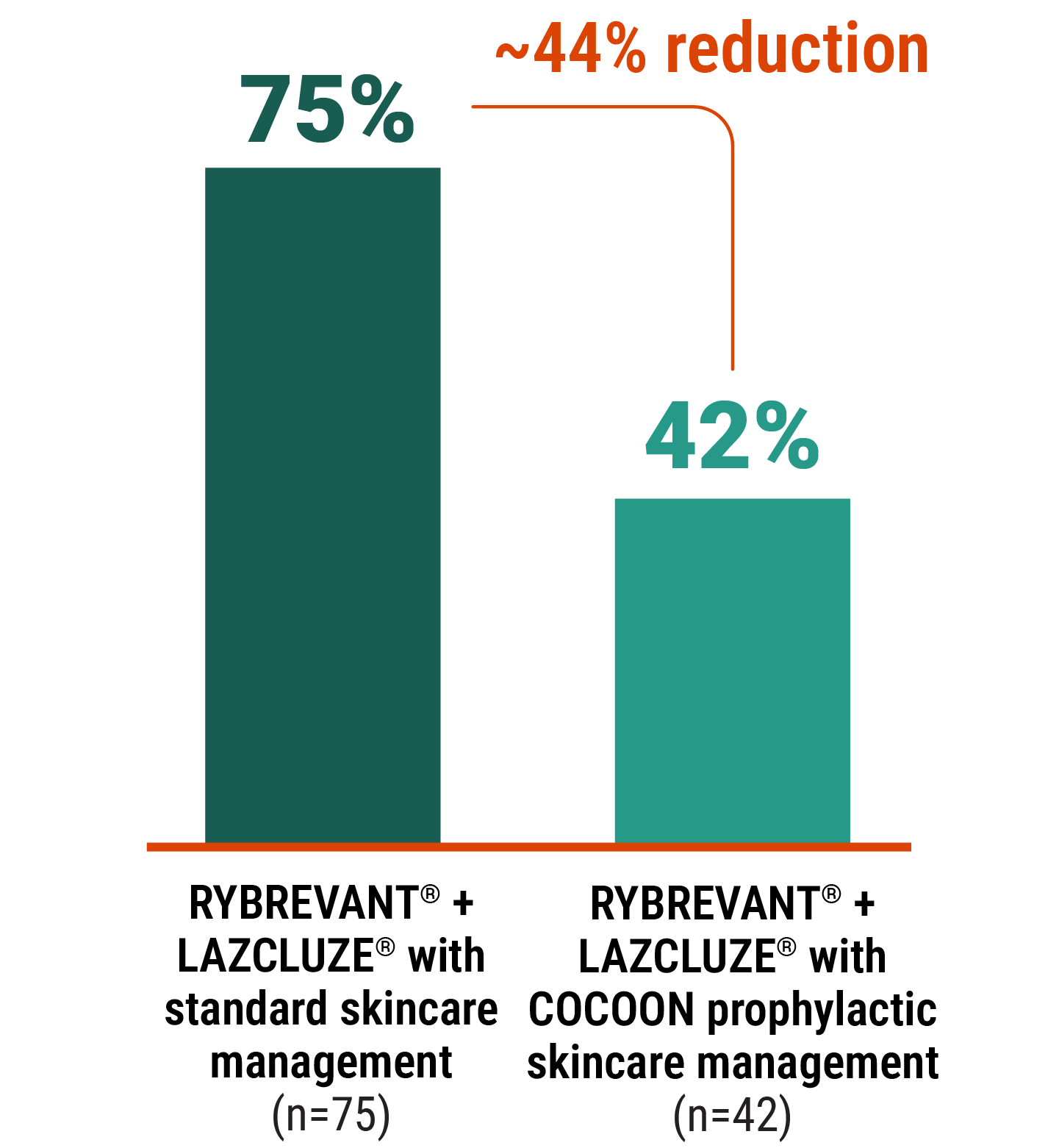
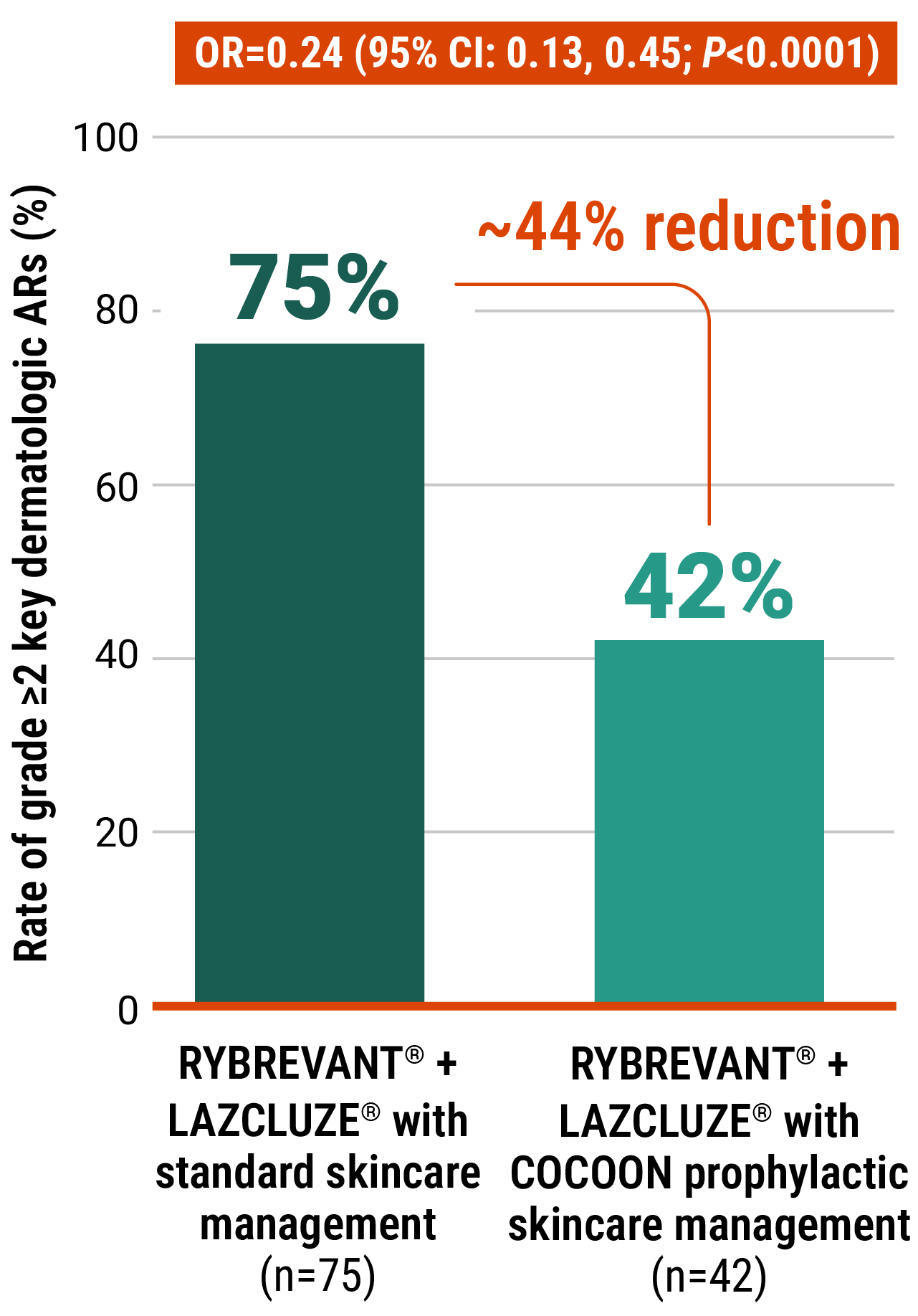
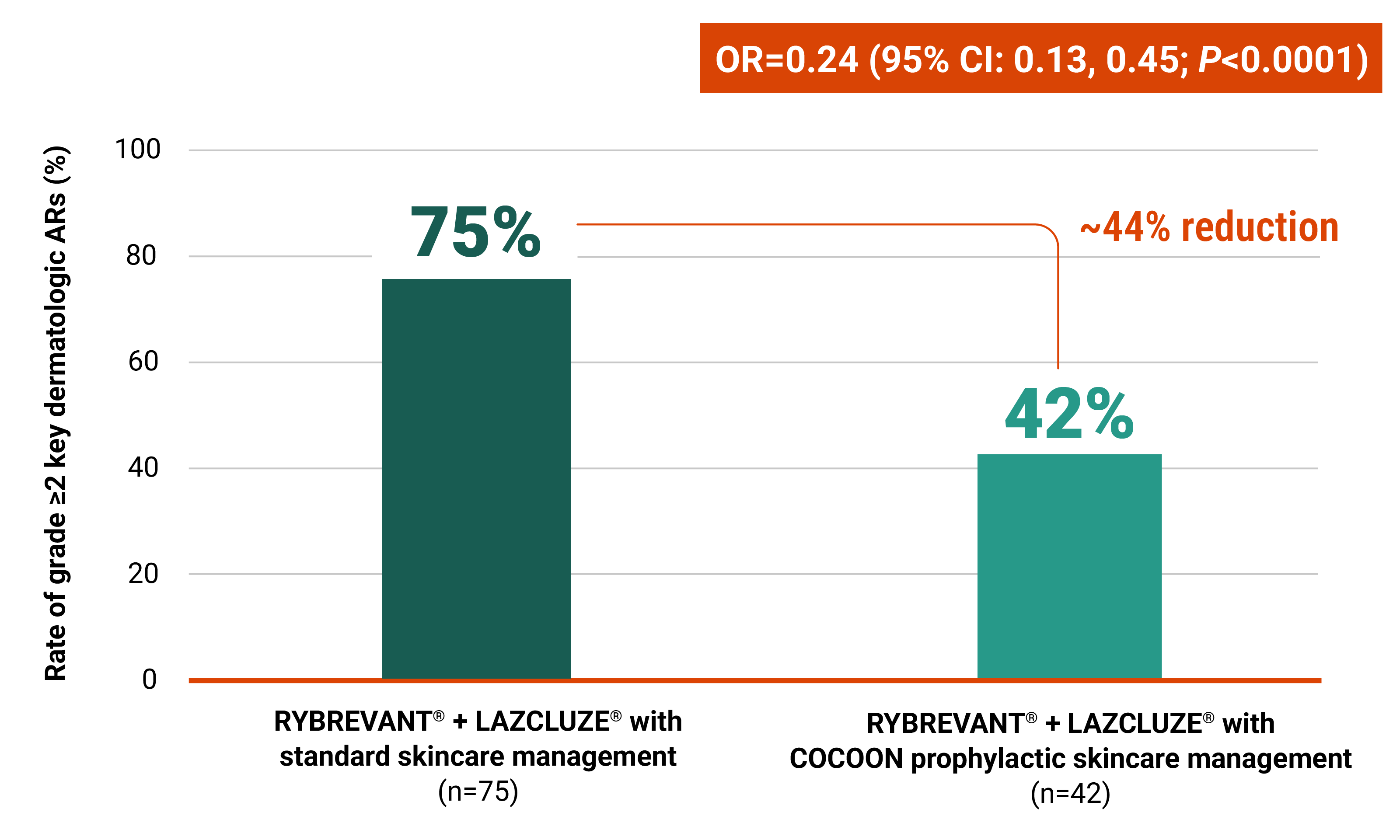
Initiate prophylactic antibiotics with skincare management to reduce the risk of dermatologic ARs
COCOON is a phase 2, open-label, multicenter, randomized study evaluating the effect of enhanced (N=99) vs standard (N=100) dermatologic management strategies in patients treated with RYBREVANT® + LAZCLUZE® in 1L. The primary endpoint is incidence of grade ≥2 dermatologic ARs of interest in the first 12 weeks after treatment initiation.2
1L, first-line.
COCOON prophylactic skincare management includes easily accessible interventions2,5
Months 1–3

Oral antibiotic
Doxycycline or minocycline
100 mg
twice daily
Months 4–12

Topical antibiotic lotion
Topical clindamycin 1% lotion on the scalp before bedtime
Daily

Moisturizer
Ceramide-based moisturizer on the body and face at least once daily
Ceramide-based, moisturizer on the body and face at least once daily

Limit direct exposure to sunlight
Wear protective clothing and broad-spectrum sunscreen (SPF ≥30)
Wear protective clothing and broad-spectrum sunscreen (SPF ≥30)

Antiseptic skin cleanser
Chlorhexidine 4% wash on fingernails and toenails for paronychia
At the time of prespecified interim analysis, COCOON prophylactic skincare management significantly reduced the incidence of grade ≥2 dermatologic ARs vs standard skincare management2
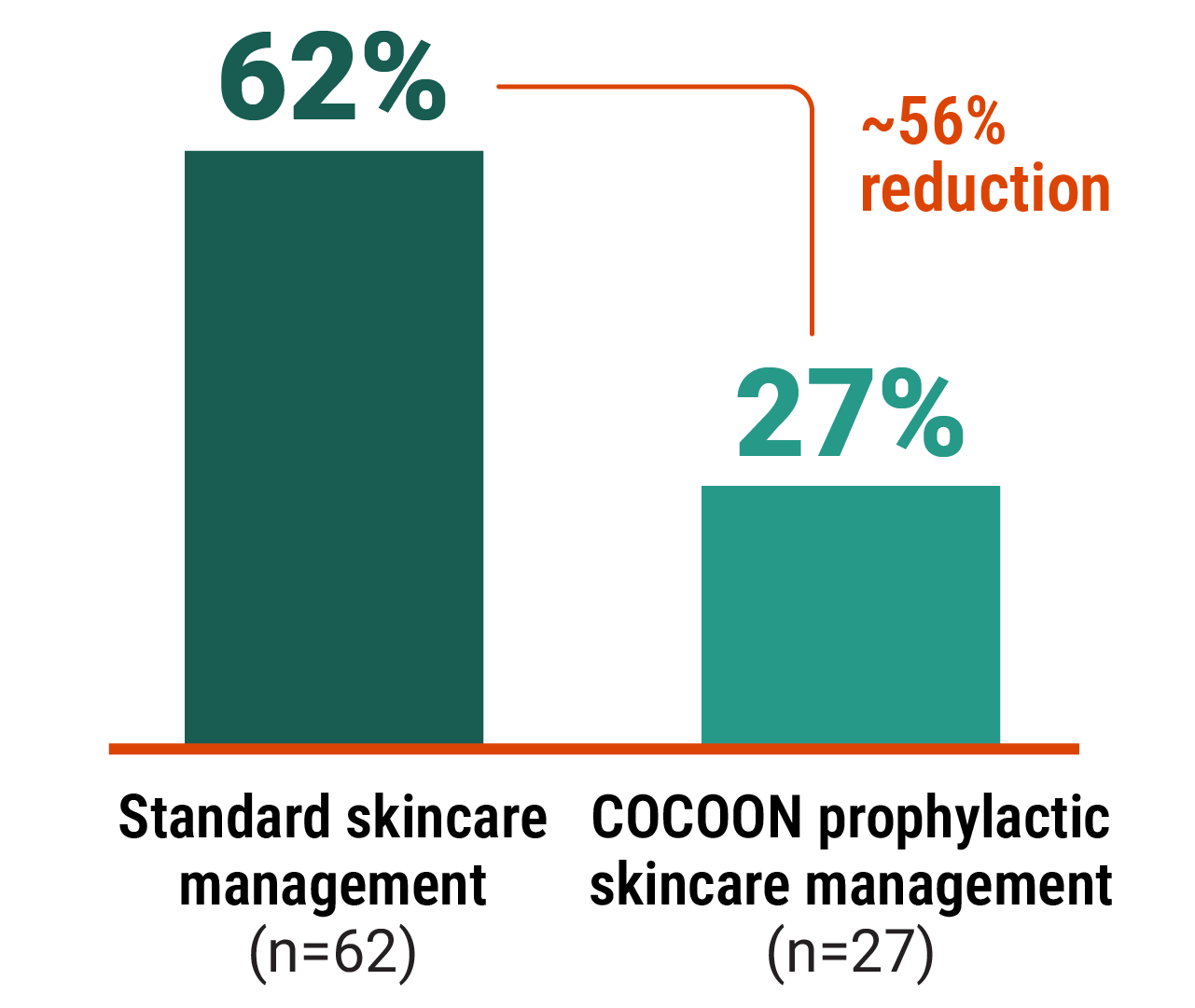
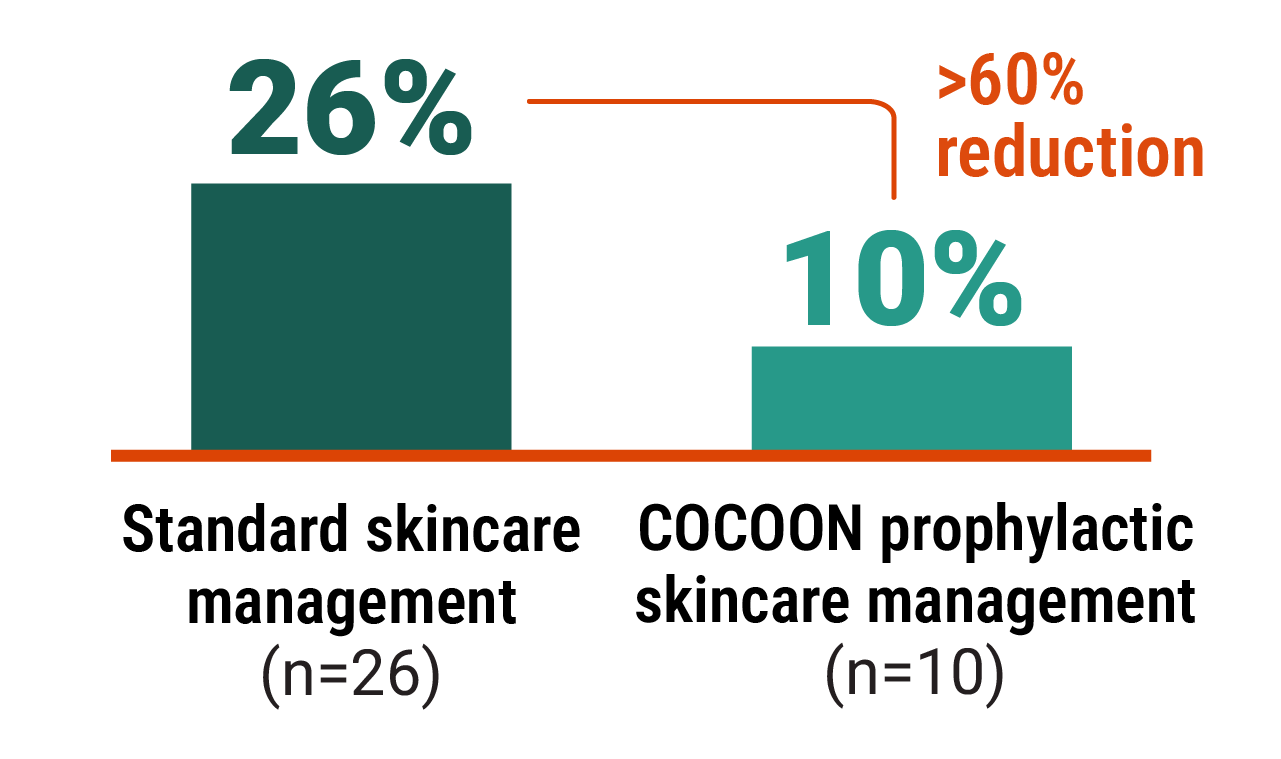
Improvements seen with the COCOON prophylactic skincare management across areas of interest2
~56% reduction in skin rash
(excluding paronychia)
>60% reduction in scalp rash
Paronychia was observed in 23% of patients receiving standard skincare management vs 21% of patients receiving COCOON prophylactic skincare management (OR=0.9 [95% CI: 0.46, 1.76]).2
CI, confidence interval; OR, odds ratio.
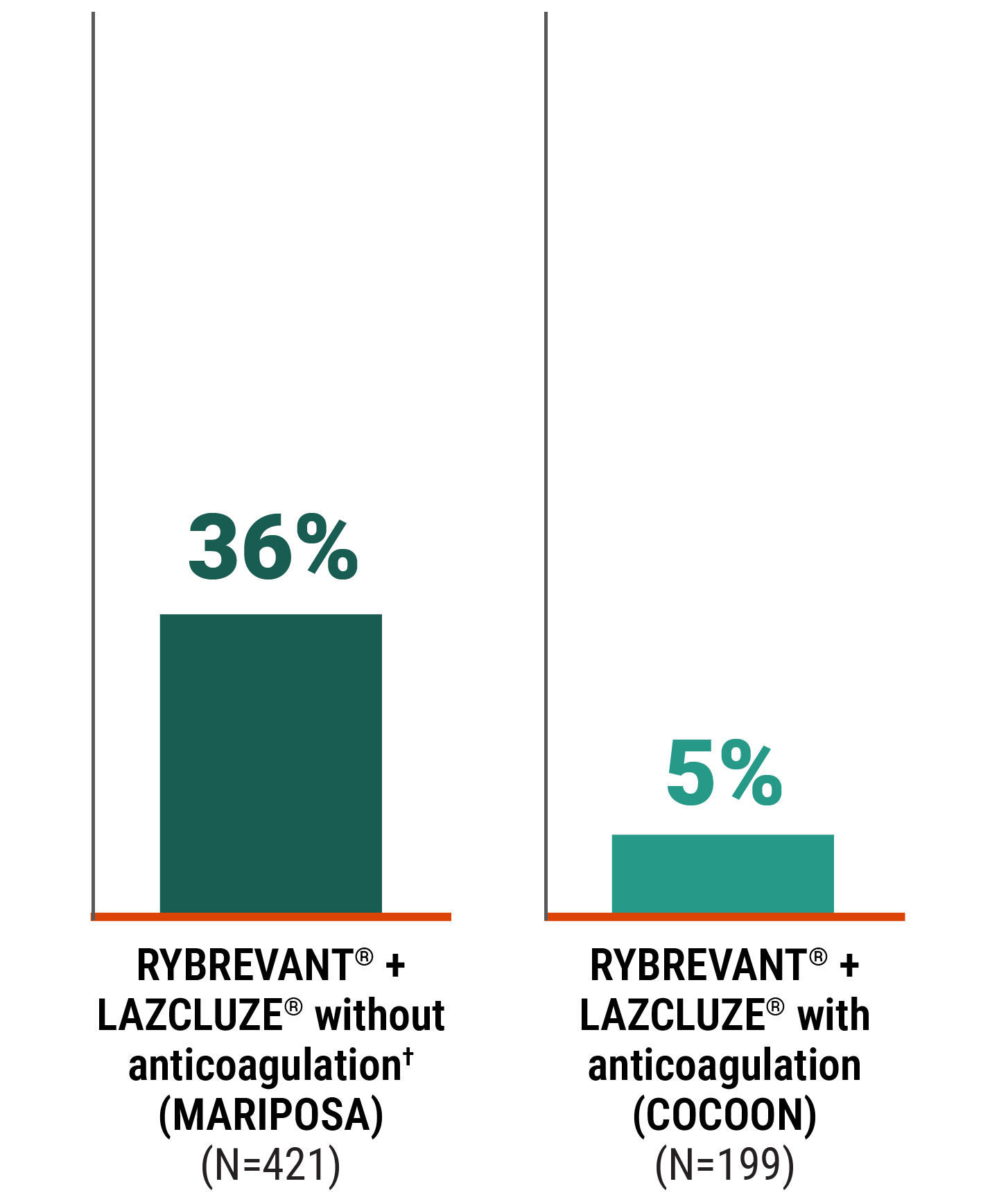
Initiate anticoagulants to reduce risk of VTE
COCOON is the first trial that required 4 months of prophylactic anticoagulation at treatment initiation, leading to a low incidence of VTE2
*Among all COCOON study participants, the VTE incidence was 11% (n=18/170) from 5 to 8 months.2
Drug-related prophylaxis for VTE5
Prophylactic treatment with an anticoagulation medicine is recommended for the first 4 months of treatment with RYBREVANT® + LAZCLUZE®.
- The use of vitamin K antagonists is not recommended
- If there are no signs or symptoms of VTE during the first 4 months of treatment, consider discontinuation of anticoagulant prophylaxis at the discretion of the healthcare provider
NSCLC, non–small cell lung cancer.

VTE, which includes DVT and PE, is a key cause of morbidity among all patients with lung cancer9
People living with cancer have a baseline risk of developing VTE that is 9 times the risk of the general population.10
NCCN Guideline recommendations for cancer-associated VTE disease6
Anticoagulant options for VTE prophylaxis for ambulatory patients with cancer include direct oral anticoagulants (DOACs) and low molecular weight heparins (LMWHs).6*†‡
*Recommendations derived from clinical trials of ambulatory patients with cancer with high thrombosis risk (>18 years, Khorana VTE Risk Score of ≥2, initiating new course of chemotherapy) and are not included in product labeling. Prophylaxis duration should be 6 months or longer if risk persists.6
†Refer to the NCCN Guidelines® for the comprehensive and most up-to-date recommendations on cancer-associated VTE when considering prophylaxis.6
‡When using RYBREVANT® in combination with LAZCLUZE®, please refer to the Prescribing Information for VTE prophylaxis recommendation.
DVT, deep vein thrombosis; PE, pulmonary embolism.
References:
- Data on file. Janssen Biotech, Inc.
- Cho BC, Li W, Spira AI, et al. Enhanced versus standard dermatologic management with amivantamab-lazertinib in EGFR-mutated advanced NSCLC: the COCOON global randomized controlled trial. J Thorac Oncol. 2025;20(10):1517-1530. doi:10.1016/j.jtho.2025.07.117
- Spira AI, Paz-Ares L, Han J-Y, et al. Preventing infusion-related reactions with intravenous amivantamab—results from SKIPPirr, a phase 2 study: a brief report. J Thorac Oncol. 2025;20(6):809-816. doi:10.1016/j.jtho.2025.01.018
- RYBREVANT FASPRO™ [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- RYBREVANT® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Cancer-Associated Venous Thromboembolic Disease V.3.2025 © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed November 6, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- Cho BC, Lu S, Felip E, et al; MARIPOSA Investigators. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. Supplementary Appendix. N Engl J Med. 2024;391(16):1486-1498.
- Yang R, Wang H, Liu D, Li W. Incidence and risk factors of VTE in lung cancer: a meta-analysis. Ann Med. 2024;56(1):1-14. doi:10.1080/07853890.2024.2390200
- Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol. 2020;38(5):496-520. doi:10.1200/JCO.19.01461
- Mulder FI, Horváth-Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959-1969. doi:10.1182/blood.2020007338