RYBREVANT® (amivantamab-vmjw) + LAZCLUZE® (lazertinib)FIRST-LINE EGFR+ mNSCLC (MARIPOSA) EFFICACY & SAFETY

Overall Survival – Secondary Endpoint
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
Unmatched survival: RYBREVANT® + LAZCLUZE® delivers superior overall survival vs osimertinib with proven durability1,2
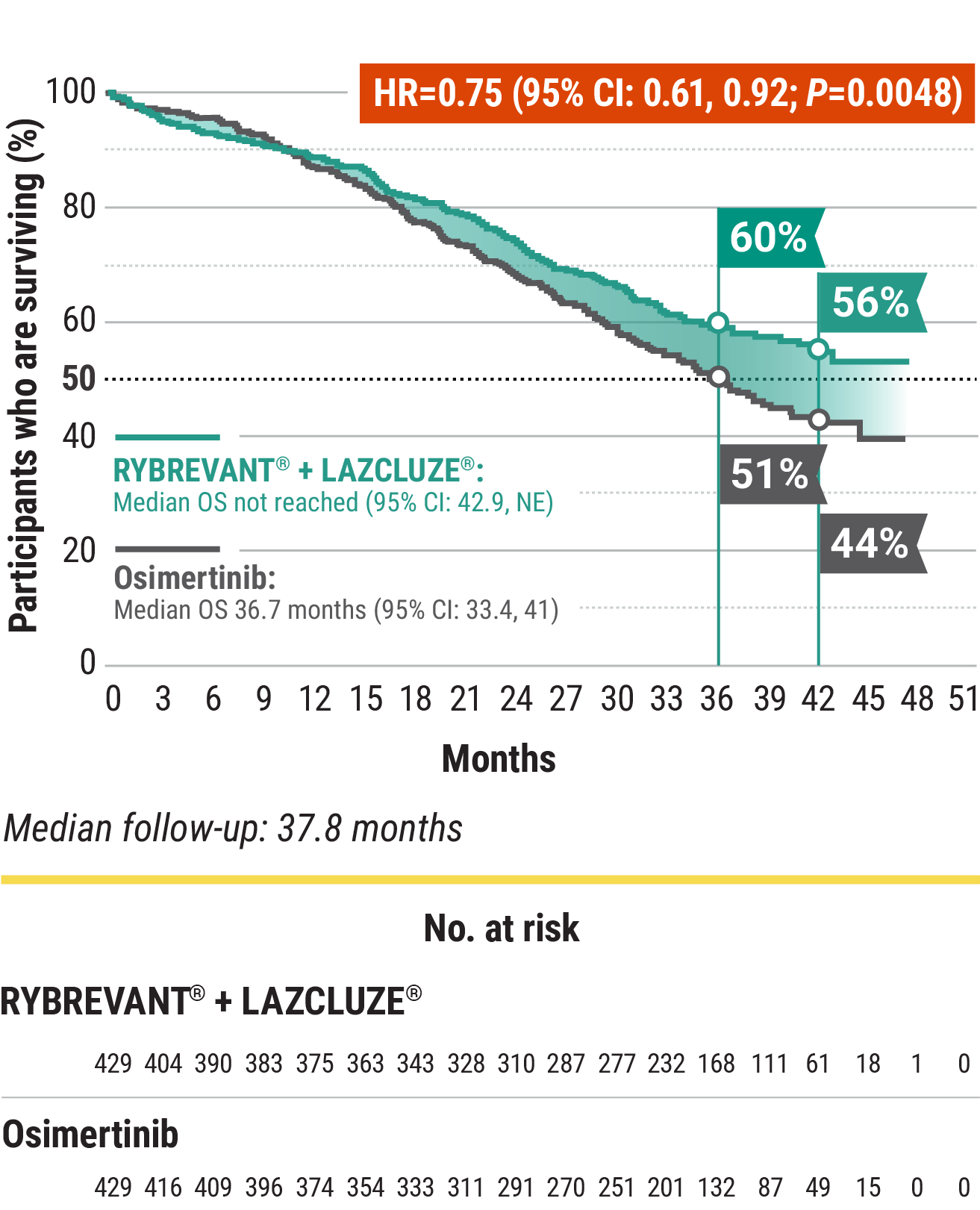
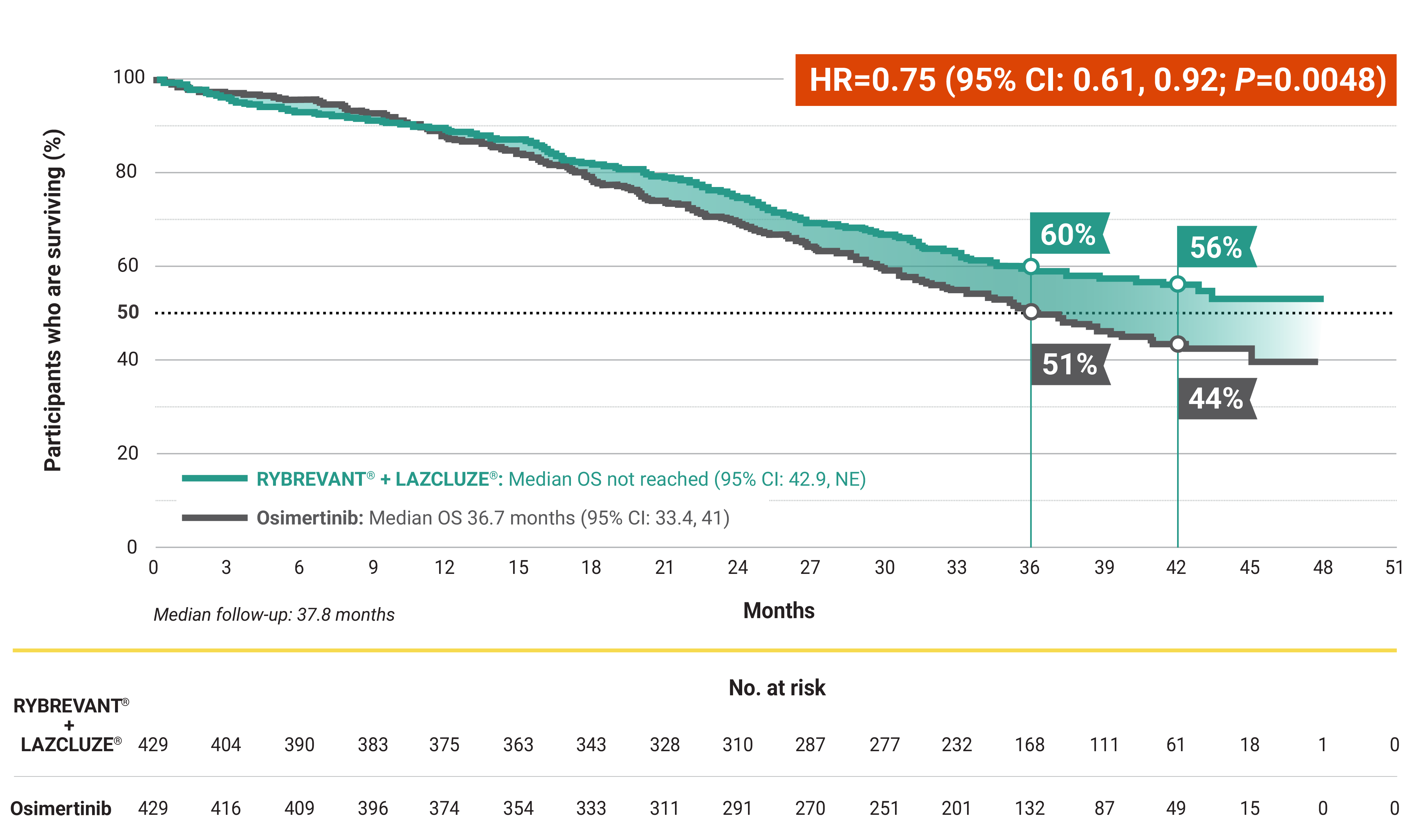
Median overall survival not reached with RYBREVANT® + LAZCLUZE® and projected to exceed 4
years1,3
Based on modeling using observed HR and mOS in the osimertinib group, assuming exponential distribution of OS in both arms. The baseline factors were: mutation type, race, brain metastases, age, sex, ECOG PS, and weight. This is a conservative estimate; final results may vary.3
CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; HR, hazard ratio; mNSCLC, metastatic non–small cell lung cancer; mOS, median overall survival; NE, not estimable; NSCLC, non–small cell lung cancer; OS, overall survival.
Progression-Free Survival – Primary Endpoint
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
Superior PFS vs osimertinib with a chemo-free combination1,4
RYBREVANT® + LAZCLUZE® demonstrated a statistically significant reduction in the risk of progression or death by 30% vs osimertinib1,5
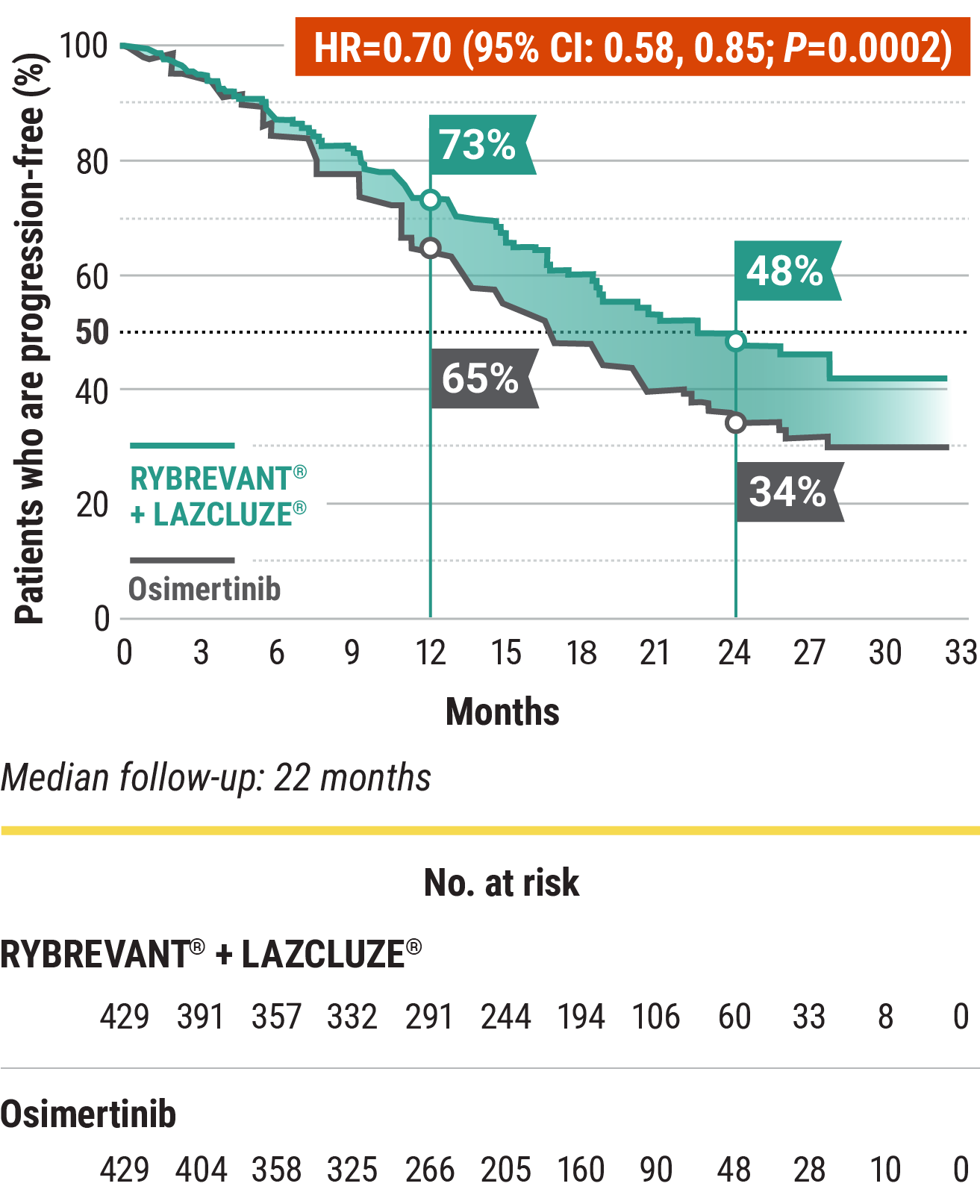
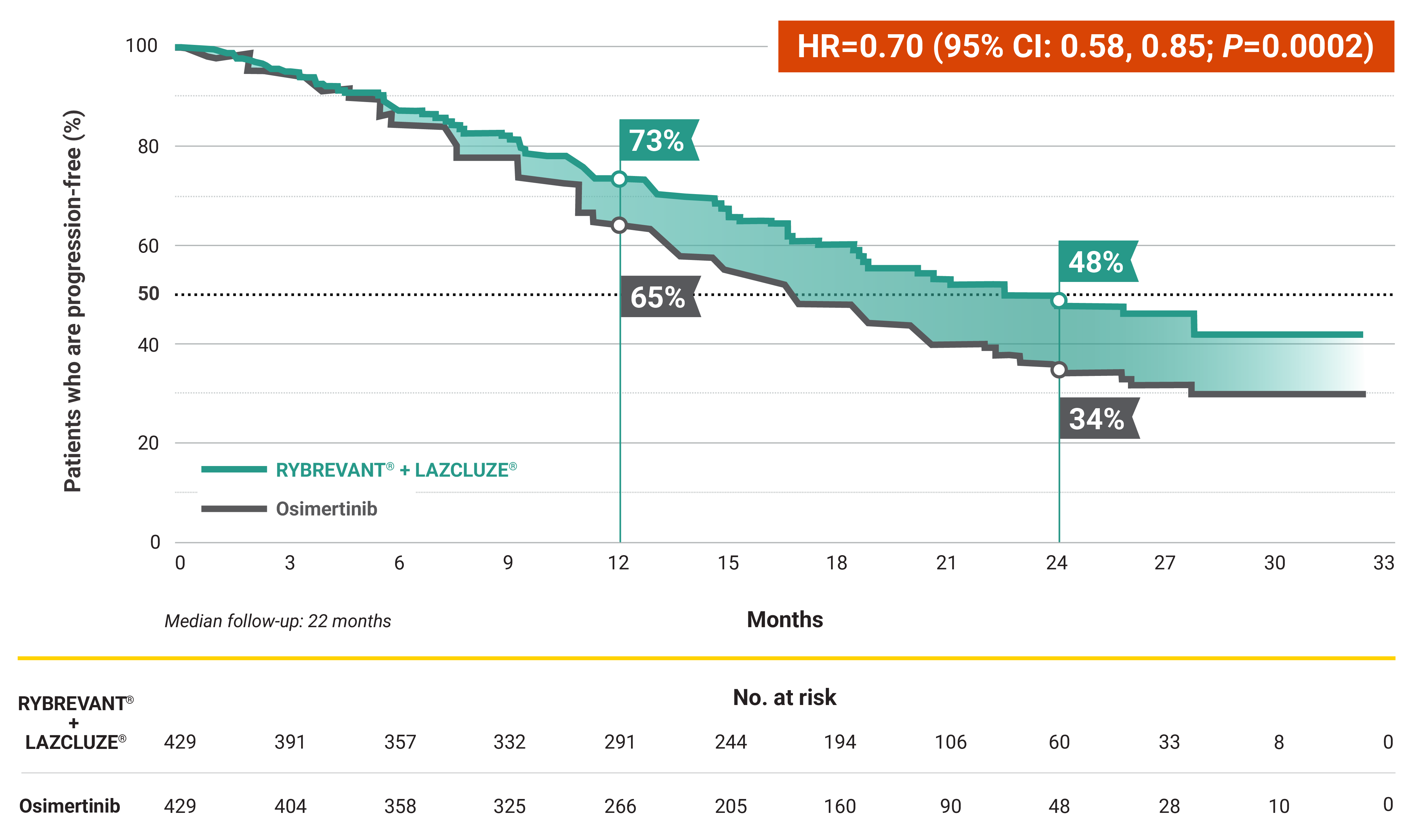
7.1-month improvement in mPFS vs osimertinib1
- 23.7-month (95% CI: 19.1, 27.7) mPFS with RYBREVANT® + LAZCLUZE® vs 16.6-month (95% CI: 14.8, 18.5) mPFS with osimertinib
*EGFR mutation discovered prior to first-line systemic therapy.6
†Amivantamab includes both amivantamab and hyaluronidase-lpuj (RYBREVANT FASPRO™) subcutaneous injection and IV amivantamb-vmjw (RYBREVANT®). Amivantamab and hyaluronidase-lpuj has different dosing and administration instructions compared with IV amivantamab-vmjw.6
‡EGFR exon 19 deletion or exon 21 L858R mutations.6
§See the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for detailed recommendations, including other treatment options.
||Prophylactic anticoagulation is recommended at the time of initiation to prevent venous thromboembolic events.6
PFS results in prespecified subgroups5
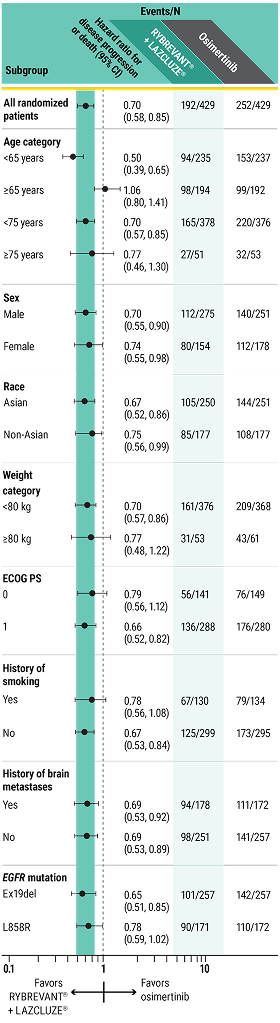
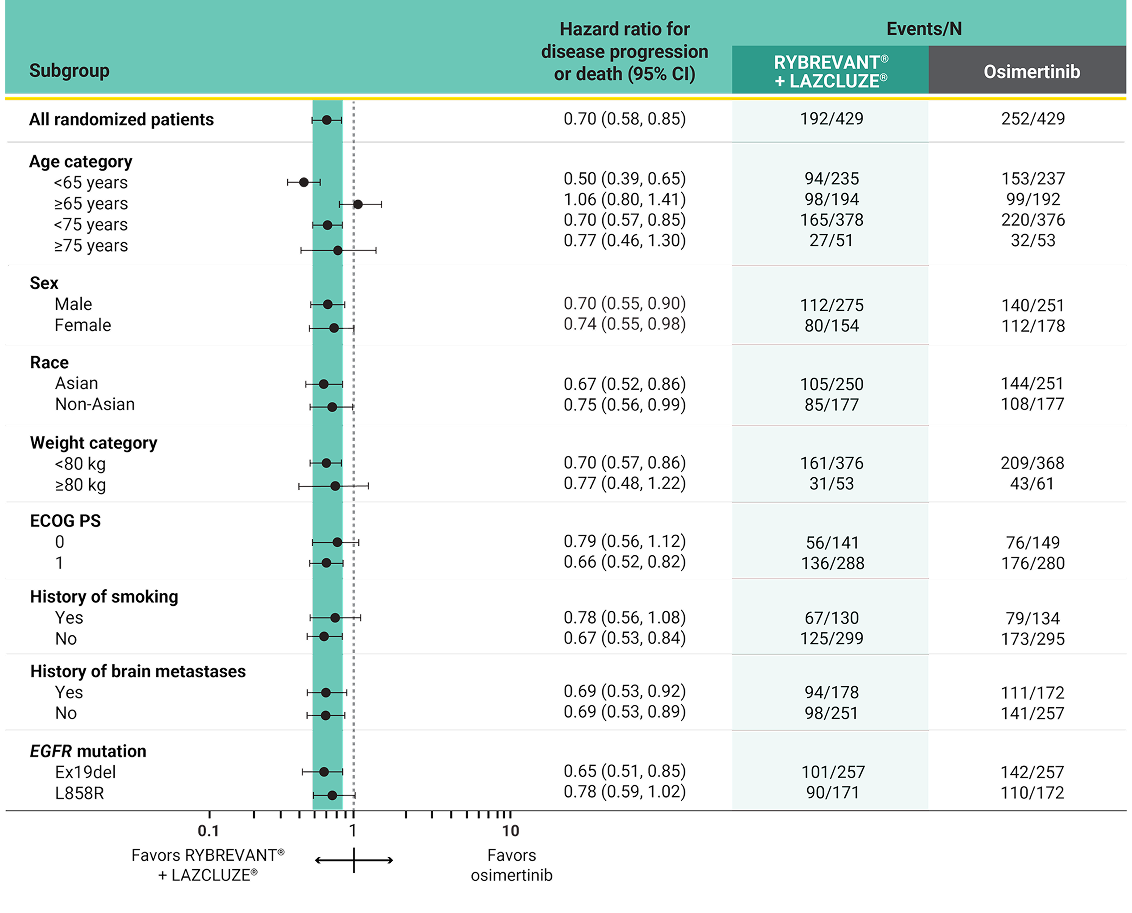
This was a prespecified analysis and was not powered to show statistical significance.
High-risk features at baseline were identified in 89% of patients with baseline ctDNA available for NGS of pathogenic alterations (N=636)5,7,8


This analysis is not included in the Prescribing Information for RYBREVANT® or LAZCLUZE®. This was a post hoc exploratory analysis and was not powered to show statistical significance.
*In MARIPOSA, pathogenic alterations were identified by NGS using ctDNA from blood with Guardant360 CDx at baseline. Ex19del and L858R ctDNA in blood was analyzed at baseline with Biodesix ddPCR. This exploratory analysis included all randomized patients who had 1 or more biomarker assessments. Subgroup analyses of efficacy endpoints were carried out using statistical methods for the primary analysis of the general MARIPOSA population.8
†Consistent results were seen in patients with detectable ctDNA using NGS (HR=0.71 [95% CI: 0.57, 0.89]).8
ctDNA, circulating tumor DNA; ddPCR, droplet digital polymerase chain reaction; DNA, deoxyribonucleic acid; ECOG PS, Eastern Cooperative Oncology performance status; ex19del, exon 19 deletion; IV, intravenous; mPFS, median progression-free survival; NE, not estimable; NGS, next-generation sequencing; PFS, progression-free survival; TP53, tumor protein p53.
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
High and durable responses with a chemo-free combination1,4
Overall response rate1
- ORR was 78% (95% CI: 74, 82) with RYBREVANT® + LAZCLUZE® (N=429) and 73% (95% CI: 69, 78) with osimertinib (N=429)
- 73% of patients treated with RYBREVANT® + LAZCLUZE® achieved a PR and 70% of patients treated with osimertinib
- 5.4% of patients treated with RYBREVANT® + LAZCLUZE® achieved a CR and 3.5% of patients treated with osimertinib
This was a prespecified analysis and was not powered to show statistical significance.
Duration of response1
Median duration of response


This was a prespecified analysis and was not powered to show statistical significance.
~1.5X mDOR with RYBREVANT® + LAZCLUZE®1
CR, complete response; mDOR, median duration of response; ORR, overall response rate; PR, partial response.
CNS Data
NCCN recommends
Amivantamab-vmjw (RYBREVANT®)-based regimens*: The only NCCN preferred combination options for brain metastases in patients with EGFR+† mNSCLC9,10‡
Intracranial PFS§ at 36 months in patients with intracranial lesions at baseline3


This was a prespecified secondary analysis and was not powered to show statistical significance.
2X intracranial PFS at 36 months with RYBREVANT® + LAZCLUZE®3
*Including but not limited to amivantamab-vmjw + lazertinib.9
†EGFR exon 19 deletion or exon 21 L858R mutations.9
‡See the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for detailed recommendations, including other treatment options.
§Based on median follow-up of 37.8 months.3
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
High intracranial ORR with durable intracranial DOR3,11
Intracranial ORR in patients with intracranial lesions at baseline*
- Intracranial ORR was 78% (95% CI: 71, 84) with RYBREVANT® + LAZCLUZE® (N=180) and 77% (95% CI: 71, 83) with osimertinib (N=186)3
- Intracranial CR was 64% with RYBREVANT® + LAZCLUZE® and 59% with osimertinib11
- Intracranial PR was 14% with RYBREVANT® + LAZCLUZE® and 19% with osimertinib11
This was a prespecified exploratory analysis and was not powered to show statistical significance.
Intracranial DOR in confirmed responders with intracranial lesions at baseline11*†
Median intracranial duration of response

This was a prespecified exploratory analysis and was not powered to show statistical significance.
~1.5X intracranial DOR with RYBREVANT® + LAZCLUZE®11
*Based on median follow-up of 37.8 months.3
†Based on subgroup of subjects with history of brain metastasis. CR and PR do not have to be confirmed.11
‡Including but not limited to amivantamab-vmjw + lazertinib.9
§EGFR exon 19 deletion or exon 21 L858R mutations.9
CNS, central nervous system; DOR, duration of response.
Study Design
For first-line treatment of adult patients with locally advanced or metastatic EGFR+ NSCLC
MARIPOSA: Evaluating the first and only multitargeted combination in first-line EGFR+ mNSCLC vs osimertinib1,4
MARIPOSA is an active-controlled, multicenter, phase 3 trial. Patients with asymptomatic or previously treated and stable intracranial metastases were eligible to enroll. Patients received treatment until disease progression or unacceptable toxicity. The evaluation of efficacy relied upon comparison between RYBREVANT® in combination with LAZCLUZE®, and osimertinib.1,5
Serial brain MRIs were conducted on all patients to assess intracranial progression and response5
- Serial brain MRIs were performed at baseline and either every 8 weeks for the first 30 months and every 12 weeks thereafter (for patients with a history of brain metastases) or every 24 weeks (for patients without a history)
The largest phase 3 trial and the only one that required serial brain MRIs for all patients, providing accurate detection of CNS progression in patients with 1L EGFR+ disease5,7,12-22*


LAZCLUZE® monotherapy arm was included to assess the contribution of the components.5
*MARIPOSA is the largest phase 3 trial that evaluated 1L treatment in patients with EGFR+ mNSCLC as of April 2025.5,12-22
Baseline characteristics were well-balanced across treatment types5


*Other includes American Indian or Alaska Native, Black, Native Hawaiian or Pacific Islander, multiple, and unknown.
†One patient in the RYBREVANT® + LAZCLUZE® arm had both ex19del and L858R.
1L, first-line; BICR, blinded independent central review; MRI, magnetic resonance imaging; RECIST, Response Evaluation Criteria in Solid Tumors.
Safety
Majority of ARs in the MARIPOSA trial were grades 1 and 21
ARs (≥10%) in patients in MARIPOSA1

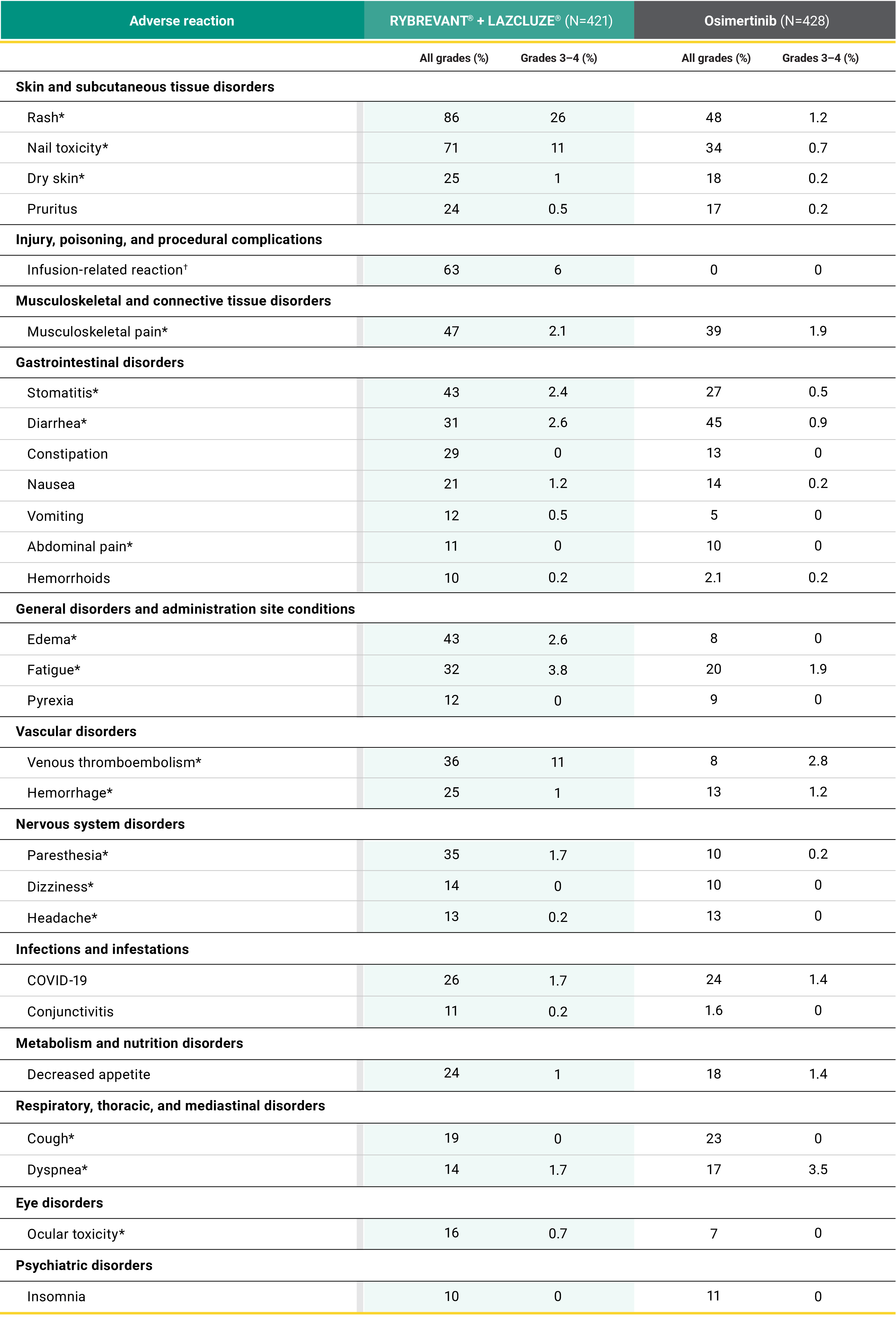
*Grouped terms.
†Applicable for RYBREVANT® only.
- Serious ARs occurred in 49% of patients with RYBREVANT® + LAZCLUZE® and 33% with osimertinib1,5
- Serious ARs in ≥2% of patients included VTE (11%), pneumonia (4%), rash (2.9%), ILD/pneumonitis (2.9%), COVID-19 (2.4%), pleural effusion (2.1%), and IRR (2.1%)1
- Fatal ARs occurred in 7% of patients who received RYBREVANT® + LAZCLUZE® and 7% with osimertinib1,5
- The most common ARs (≥20%) were rash, nail toxicity, IRR, musculoskeletal pain, stomatitis, edema, VTE, paresthesia, fatigue, diarrhea, constipation, COVID-19, hemorrhage, dry skin, decreased appetite, pruritus, and nausea1
- Clinically relevant ARs (<10%) in patients who received RYBREVANT® + LAZCLUZE® included skin ulcer (5.2%) and ILD/pneumonitis (3.1%)1,11
Learn about the safety profile of RYBREVANT FASPRO™
Learn moreSelect laboratory abnormalities that worsened from baseline (≥20%) in MARIPOSA1*


*The denominator used to calculate the rate is the number of patients with a baseline value and at least one post-treatment value for the specific lab test.
The most common grade 3 or 4 laboratory abnormalities (≥2%) were decreased albumin, decreased sodium, increased alanine aminotransferase, decreased potassium, decreased hemoglobin, increased aspartate aminotransferase, increased gamma-glutamyl transferase, and increased magnesium.1


This was a post hoc exploratory analysis and is not included in the Prescribing Information for RYBREVANT® or LAZCLUZE®.
*Patients with PFS events or who were censored in the first 4 months were excluded from this analysis.
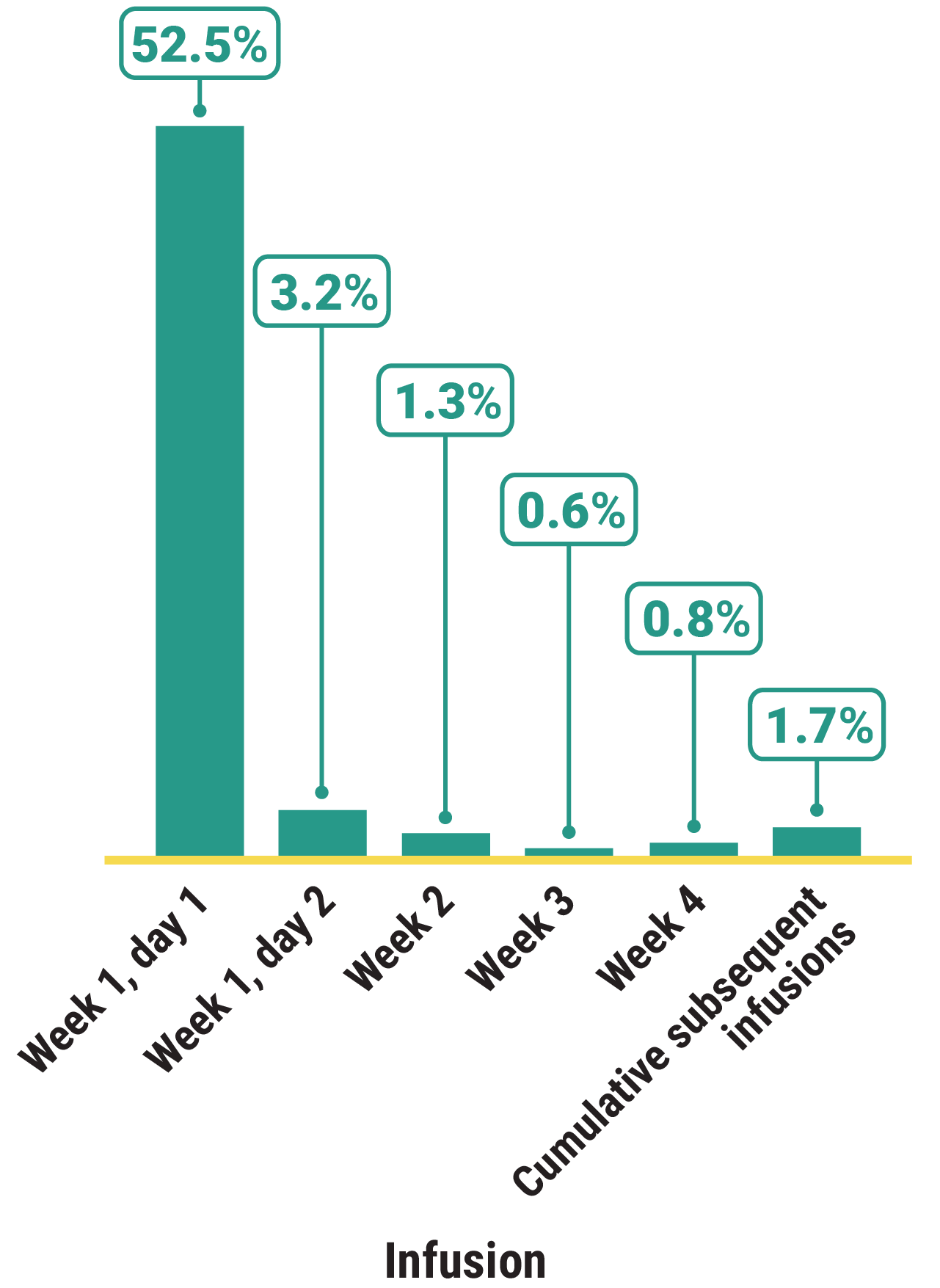

- 92.3% of IRRs were grades 1 and 211
- Median time to onset of first IRR was 1 hour (range, 0.05–52.5 hours)11
- Monitor patients for any signs and symptoms of IRRs during RYBREVANT® infusion in a setting where cardiopulmonary resuscitation medication and equipment are available. Interrupt infusion if IRR is suspected. Reduce the infusion rate or permanently discontinue RYBREVANT® based on severity10
- If an anaphylactic reaction occurs, permanently discontinue RYBREVANT®10
- Signs and symptoms of IRR include dyspnea, flushing, fever, chills, nausea, chest discomfort, hypotension, and vomiting10
Prophylaxis may reduce the risk of IRRs, dermatologic ARs, and VTE
Learn moreAR, adverse reaction; ILD, interstitial lung disease; IRR, infusion-related reaction; VTE, venous thromboembolism.
Dose Modifications and Discontinuation Rates
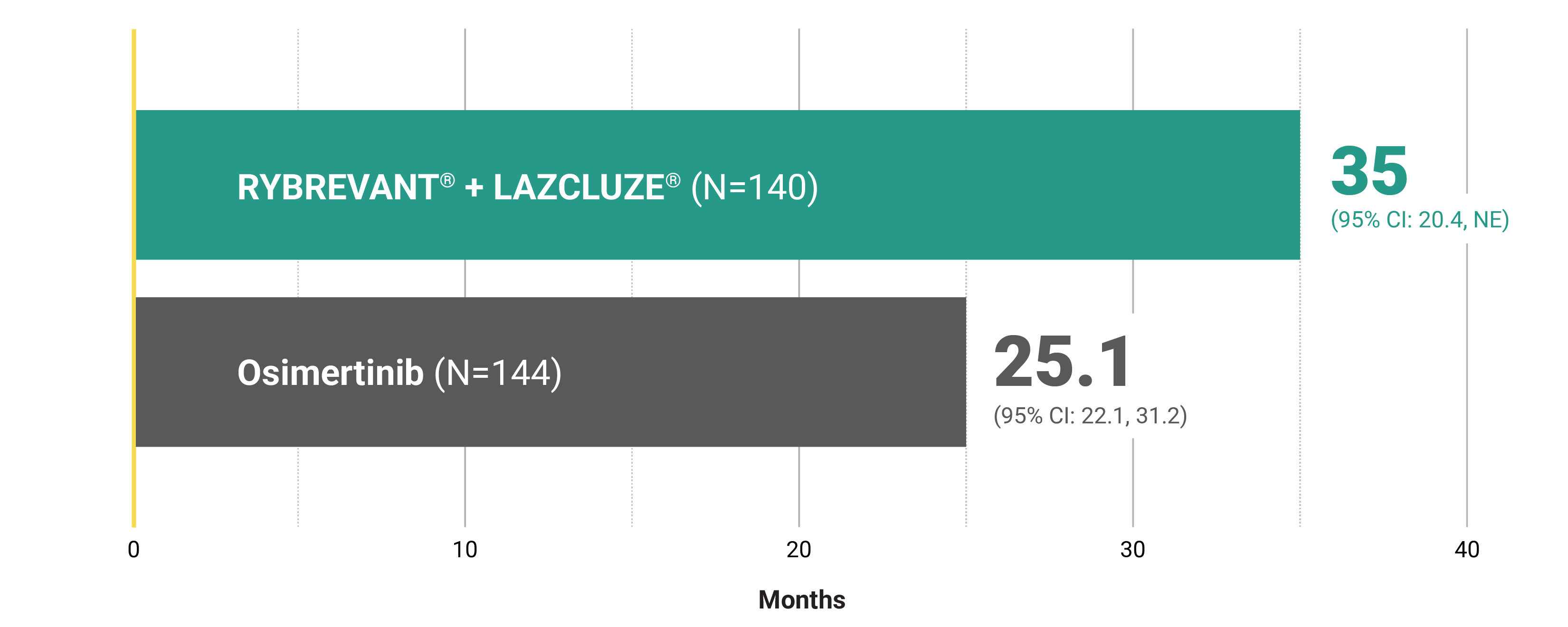
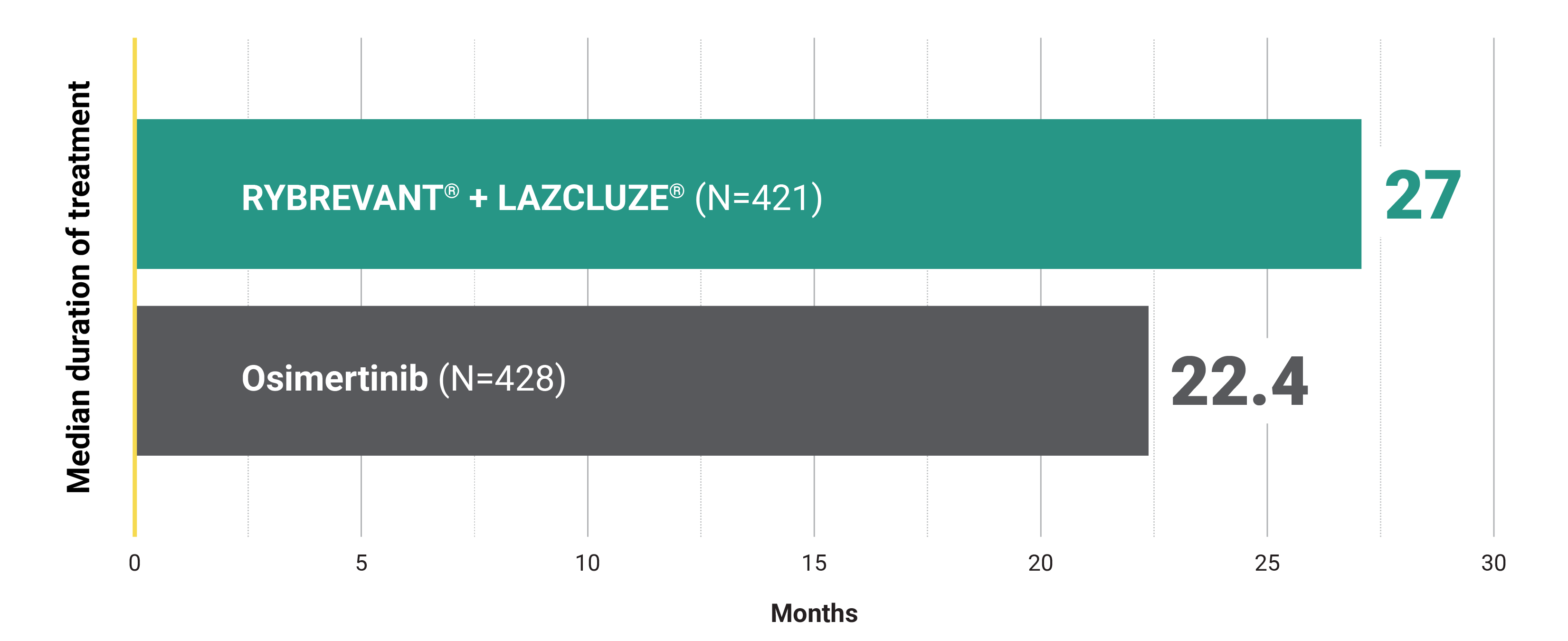
Adaptable dosing is available to help your patients manage ARs and stay on treatment11*
Median duration of treatment including dose modifications3

*Certain types and severity of ARs require discontinuation after first occurrence.1
With dose interruptions in the first 4 months:
27.5 months
(95% Cl: 20.3, NE) (N=188)
Without interruptions in the first 4 months:
25.7 months
(95% Cl: 22.2, NE) (N=190)
- In this analysis, dose interruption was defined as a skipped dose that is not made up; this population may also include patients who had a dose reduction or drug discontinuation23
This was a post hoc exploratory analysis from MARIPOSA and is not included in the Prescribing Information for RYBREVANT® or LAZCLUZE®.
*In this descriptive analysis of PFS, the hazard ratio by multivariable analysis (via multivariate Cox proportional hazards model, only included patients still at risk of PFS at 4 months) adjusted for age, ECOG PS, EGFR mutation type, Asian race, and history of brain metastases was 1.06 (95% CI: 0.73, 1.44).23
†To minimize bias, outcomes (such as progression events or deaths that could occur before interruptions leading to outcomes-based selection bias) were evaluated after the first 4 months. Patients who discontinued the study, had disease progression, or died in the first 4 months were not evaluated, as they were not in the study by the cutoff timepoint (and the outcome event may have occurred prior to the interruption).23
Dose modifications1,4
- Dose interruptions due to an AR occurred in 88% of patients with RYBREVANT® and 72% of patients with LAZCLUZE®
- Dose reductions due to an AR occurred in 46% of patients with RYBREVANT® and 42% of patients with LAZCLUZE®
Discontinuation rates
- The rate of discontinuations of all agents due to treatment-related ARs was 10% for RYBREVANT® + LAZCLUZE®5
- Permanent discontinuation of RYBREVANT® due to an AR occurred in 34% of patients1
- Permanent discontinuation of LAZCLUZE® due to an AR occurred in 21% of patients4
Learn more about available adaptable dosing
Learn more2L, second-line.
References:
- RYBREVANT FASPRO™ [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Yang JC-H, Kim YJ, Lee S-H, et al. Amivantamab plus lazertinib vs osimertinib in first-line EGFR-mutant advanced NSCLC: Final overall survival from MARIPOSA. Presented at: European Lung Cancer Congress; March 26-29, 2025; Paris, France.
- Yang JC-H, Lu S, Hayashi H, et al; for the MARIPOSA Investigators. Overall survival with amivantamab–lazertinib in EGFR-mutated advanced NSCLC. N Engl J Med. 2025;393(17):1681-1693. doi:10.1056/NEJMoa2503001
- LAZCLUZE® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Cho BC, Lu S, Felip E, et al; MARIPOSA Investigators. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. N Engl J Med. 2024;391(16):1486-1498. doi:10.1056/NEJMoa2403614
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.4.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed March 6, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- Cho BC, Lu S, Felip E, et al; MARIPOSA Investigators. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. Supplementary Appendix. N Engl J Med. 2024;391(16):1486-1498. doi:10.1056/NEJMoa2403614
- Felip E, Cho BC, Gutiérrez V, et al. Amivantamab plus lazertinib versus osimertinib in first-line EGFR-mutant advanced non-small cell lung cancer with biomarkers of high-risk disease: a secondary analysis from MARIPOSA. Ann Oncol. 2024;35(9):805-816. doi:10.1016/j.annonc.2024.05.541
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Central Nervous System Cancers V.3.2025. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed December 5, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- RYBREVANT® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Data on file. Janssen Biotech, Inc.
- Yang JC-H, Wu Y-L, Schuler M, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015;16(2):141-151. doi:10.1016/S1470-2045(14)71173-8
- Wu Y-L, Cheng Y, Zhou X, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18:1454-1466. doi:10.1016/S1470-2045(17)30608-3
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239-246. doi:10.1016/S1470-2045(11)70393-X
- Nakagawa K, Garon EB, Seto T, et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(12):1655-1669. doi:10.1016/S1470-2045(19)30634-5
- Kawashima Y, Fukuhara T, Saito H, et al. Bevacizumab plus erlotinib versus erlotinib alone in Japanese patients with advanced, metastatic, EGFR-mutant non-small-cell lung cancer (NEJ026): overall survival analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Respir Med. 2022;10(1):72-82. doi:10.1016/S2213-2600(21)00166-1
- Douillard J-Y, Ostoros G, Cobo M, et al. First-line gefitinib in Caucasian EGFR mutation-positive NSCLC patients: a phase-IV, open-label, single-arm study. Br J Cancer. 2014;110(1):55-62. doi:10.1038/bjc.2013.721
- Mok TS, Wu Y-L, Thongprasert S, et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947-957. doi:10.1056/NEJMoa0810699
- Soria J-C, Ohe Y, Vansteenkiste J, et al; FLAURA Investigators. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N Engl J Med. 2018;378(2):113-125. doi:10.1056/NEJMoa1713137
- Planchard D, Jänne PA, Cheng Y, et al; FLAURA2 Investigators. Osimertinib with or without chemotherapy in EGFR-mutated advanced NSCLC. N Engl J Med. 2023;389(21):1935-1948. doi:10.1056/NEJMoa2306434
- Mok TS, Wu Y-L, Ahn M-J, et al. Osimertinib or platinum–pemetrexed in EGFR T790M–positive lung cancer. N Engl J Med. 2017;376(7):629-640. doi:10.1056/NEJMoa1612674
- Goldberg SB, Pulla MP, Lisberg AE, et al. 123TiP: TROPION-Lung14: a phase III study of osimertinib ± datopotamab deruxtecan (Dato-DXd) as first-line (1L) treatment for patients with EGFR-mutated locally advanced or metastatic (LA/M) non-small cell lung cancer (NSCLC). J Thorac Oncol. 2025;20(suppl 1):S86-S87.
- Campelo MRG, Cho BC, Girard N, et al. Effect of amivantamab dose interruptions on efficacy and safety of first-line amivantamab plus lazertinib in EGFR-mutant advanced NSCLC: exploratory analyses from the MARIPOSA study. Presented at: European Lung Cancer Congress; March 20-23, 2024; Prague, Czech Republic.